(1)
Chennai Breast Centre, Chennai, India
Breast cysts are a part of the involutionary fibrocystic changes that occur in the TDLUs and seen predominantly in the perimenopausal age group.
Cyst Formation
The ductules either involute or get compressed, while the acinar cells continue to produce fluid. This fluid accumulates resulting in micro- and macrocysts.
The cyst fluid may be:
1.
A transudate which is rich in sodium and low in potassium
2.
Secretory in nature, produced by apocrine metaplasia which is rich in potassium and low in sodium
The secretory cysts that occur in association with metaplasia often have a high incidence of recurrence.
Clinical Features
The vast majority of cysts are asymptomatic. They are incidentally seen on routine mammographic screening. Cysts are seen frequently in the 40s and early 50s (i.e., in the perimenopausal age group). They represent the involutionary changes that happen around menopause and tend to disappear after menopause. They are hormone sensitive and can reappear after menopause if HRT is used. More than 50 % of women who have cysts have bilateral and multiple cysts. They may have fluctuations in size and number in relation to cyclical changes.
Symptomatic cysts present with a palpable breast mass or masses that may develop suddenly and may be associated with pain and tenderness. Clinically detected breast mass cannot be characterized as a cyst on the basis of physical findings alone.
Mammographic Features
Mammographic findings of breast cyst are variable. They can appear as single or multiple and unilateral or bilateral masses of varying sizes. Cyst can appear as circumscribed, medium- or high-density masses (Fig. 18.1). They may be partially obscured and may exhibit changing patterns and sizes over time. A halo sign may be seen in the visible portion of the margins (Fig. 18.2). Bilateral multiple rounded medium- or high-density opacities that are close to each other are likely to be cysts (Fig. 18.3).
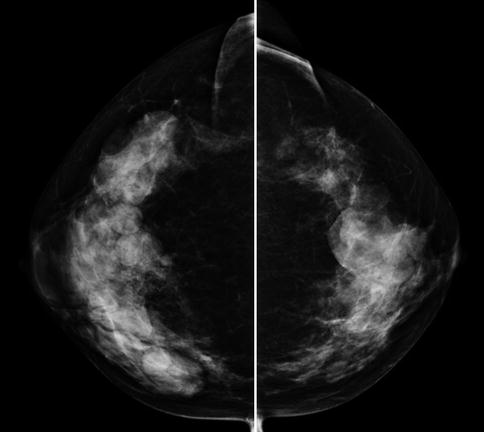
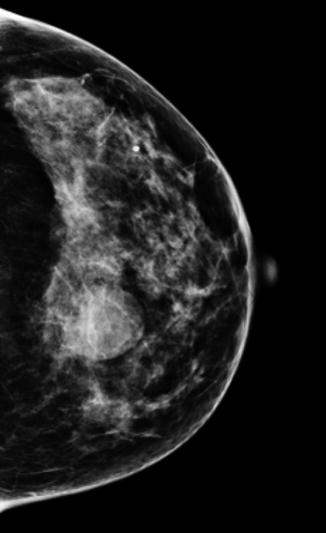
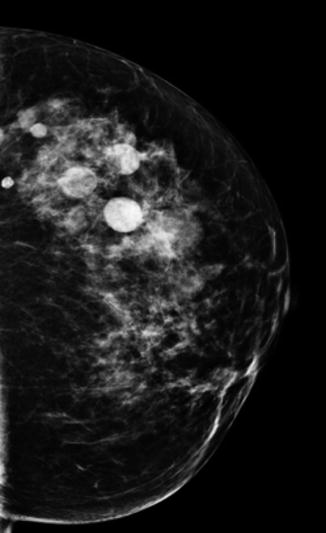
Fig. 18.1
Mammogram CC view showing multiple bilateral dense round and ovoid opacities—case of multiple cysts
Fig. 18.2
Left CC view showing rounded dense opacity with partial halo and partly obscured margins—case of cyst
Fig. 18.3
CC view showing multiple medium or high density opacities that are close to each other—cysts
Sometimes they may also present as asymmetric densities without a distinct margin, where an ultrasound would be required to evaluate further.
Calcium oxalate may be deposited in the cysts resulting in involutionary-type scattered calcifications seen on mammograms as rounded punctuate calcifications. Milk of calcium is in suspension within the microcysts. In the cranial caudal projection, they are seen as rounded clusters of calcification, but in a 90° lateromedial projection, the milk of calcium in the suspended state settles down in the bottom of the cysts taking the shape of the saucer or a tea cup (Fig. 18.4a, b). These are involutionary-type calcifications and they do require further evaluation.
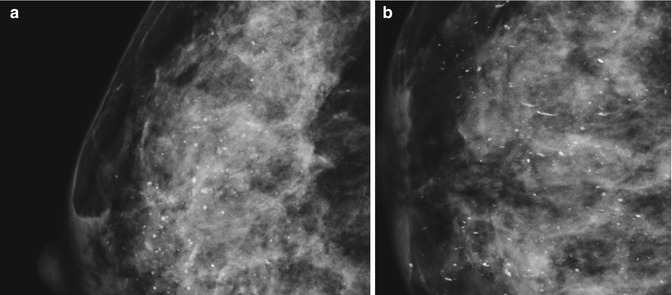
Fig. 18.4
(a) Magnified mammogram image showing multiple rounded scattered punctate calcifications. (b) 90 lateral projections in the same patient (magnified image) showing “tea cup“
Cyst wall calcifications are demonstrated as rim-like calcifications on a mammogram, and they are definitely benign and they do not warrant any further evaluation (Fig. 18.5).
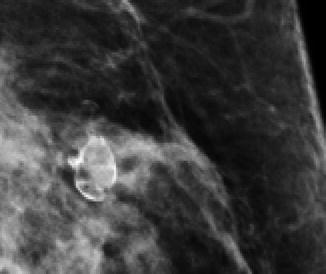
Fig. 18.5
Rim-like cyst wall calcifications
Cysts cannot be distinguished from other water density masses and malignancies on mammography and always require additional imaging with ultrasonography.
Ultrasound Features
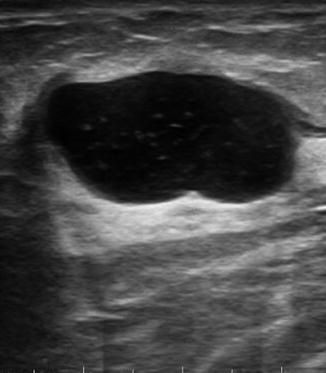
On breast ultrasound, a simple cyst is defined as a well-circumscribed, rounded, or oval anechoic mass with a thin wall and posterior acoustic enhancement (Fig. 18.6). The rapidly developing cysts may be rounded (Fig. 18.7) and tense, whereas incidentally noticed cysts on screening may be more ovoid and compressible (lazy cysts) (Fig. 18.8). With newer techniques like elastography, cysts appear soft. With the strain technique, there might be an even strain indicating a benign lesion or there is a trilaminar appearance that is typical of a cyst due to reverberation artifacts. With shear-wave technique, cysts appear black because shear waves do not propagate in fluid. Once a mass meets all the criteria for a simple cyst, it is classified as BI-RADS 2 (Fig. 18.9).
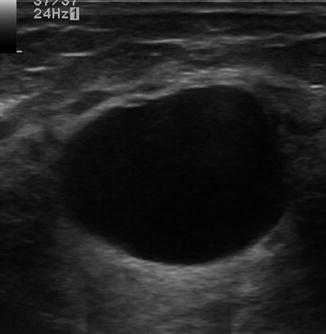
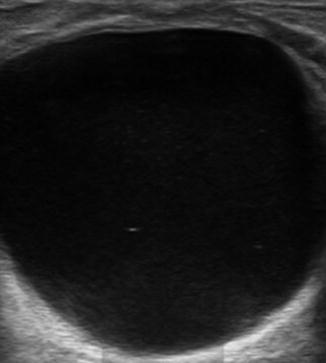

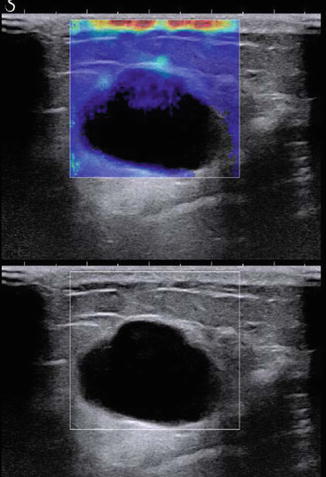
Fig. 18.6
Anechoic cyst, thin imperceptible wall, and posterior acoustic enhancement
Fig. 18.7
Round tension cyst
Fig. 18.8
Simple ovoid cyst lazy cyst
Fig. 18.9
Shear-wave elastography of a cyst. Shear waves are not conducted through fluid
Ultrasound is highly accurate in identifying simple cysts, but unfortunately not all cysts exhibit features of a simple cyst.
Management of Simple Cysts
Symptomatic, large tension cysts will require aspiration to relieve pain and anxiety, but others do not require any intervention or even follow-up. However, the woman needs to be educated to seek medical attention if anything new and palpable is felt and not to assume that it is another cyst (Fig. 18.10).
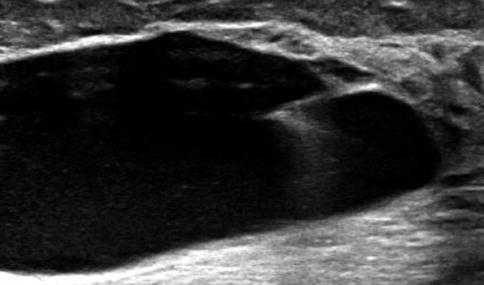
Fig. 18.10
Needle aspiration of large cyst
Complicated Cysts
A cyst that contains low-level internal echoes or fluid–fluid or fluid–debris levels (Figs. 18.11 and 18.12) that can shift with changes in the patient’s position is referred to as complicated cyst (Fig. 18.13). The causes of internal echoes within an otherwise simple cyst include cell debris, protein, cholesterol, blood, WBCs, and epithelial cells. Because complicated cysts do not meet the criteria of a simple cyst, they cannot be given a BI-RADS 2 classification. Instead, a more appropriate classification is BI-RADS 3 because there is only a 0.2 % chance of malignancy. Aspiration or short-interval follow-up should be offered.