III: MANAGEMENT OF OBSTETRIC CONDITIONS (GREATER THAN VIABILITY) |
|
Fetal Evaluation and Clinical Applications | 12 |
Electronic fetal heart rate monitoring (EFM) technologies and ultrasound are the primary surveillance tools used for fetal evaluation in an obstetric triage setting. Approximately 85% of live births in the United States are assessed with EFM, making it one of the most widely used obstetric tools (Freeman, Garite, Nageotte, & Miller, 2012; Tucker, Miller, & Miller, 2009). Technologic advances have produced a machine that provides clinicians with a valuable tool to display fetal heart rate (FHR) patterns accurately. The benefits of EFM include decreased intrapartum death rates, improved Apgar scores, and the determination of well-being in the high-risk fetus. The goals of fetal evaluation are to accurately identify the well-oxygenated fetus so that unnecessary intervention is avoided as well as recognize the fetus at risk, thus preventing adverse perinatal outcomes (American College of Obstetricians and Gynecologists [ACOG], 2014; Devoe, 2008; L. A. Miller, Miller, & Cypher, 2017; Signore, Freeman, & Spong, 2009). Common maternal and fetal indications for EFM testing in an obstetric triage setting are presented in Exhibit 12.1.
EXHIBIT 12.1
Common Indications for Electronic Fetal Monitoring Evaluation in Obstetric Triage
• Postterm pregnancy
• Amniotic fluid abnormalities
• Preterm premature rupture of membranes (PPROM)
• Decreased fetal movement (DFM)
• Hypertensive disorders
• Abnormal serum markers
• Diabetes
• Multiple gestation
• Fetal growth restriction
• History of stillbirth
• Minor trauma
Sources: Adapted from ACOG (2014); L. A. Miller et al. (2017); and Signore et al. (2009).
126Despite widespread use of these technologies, there is limited evidence to guide the type of test, testing intervals, gestational ages at which to initiate testing, or optimal frequency of testing (Signore et al., 2009). Key measures of the effectiveness of a test include the false negative rate (incidence of fetal death within 1 week of normal antepartum test) and the false positive rate (abnormal test that prompts delivery of a healthy fetus; L. A. Miller et al., 2017). These rates are presented for each of the current testing methods as described in Table 12.1.
FETAL TESTING METHODS AND EVALUATION
Nonstress Test
Nonstress tests (NSTs) are often the first cardiotocographic test performed in assessing fetal well-being and are initiated for a variety of maternal and fetal conditions. The characteristics of the baseline FHR unrelated to contractions are observed with healthy fetuses displaying normal fluctuations and oscillations in the baseline. In addition, the presence of accelerations correlates with fetal well-being (Freeman et al., 2012) and normal fetal autonomic functioning (ACOG, 2014). Absence of accelerations on a baseline FHR tracing can be associated with a fetal sleep cycle, medication administration, congenital abnormalities, or adverse fetal outcomes (Signore et al., 2009) and acidosis (ACOG, 2014; Freeman et al., 2012).
Both the external tocodynamometer and the ultrasound transducer are secured to the woman’s abdomen to record uterine contractions and FHR, respectively. A separate “event marker” button is given to the mother to record perceived fetal movements. The fetal monitor tracing is recorded for 20 minutes during which clinicians can observe FHR baseline, variability, and the presence or absence of accelerations, decelerations, and contractions, along with maternal perception of fetal movements. A review of FHR nomenclature and definitions is given in Table 12.2.
Interpretation and Management
Accelerations of the FHR in response to fetal movements are the basis for interpretation and management of the NST. There is no universal agreement for defining a “reactive” NST, the number of accelerations, or the length of testing (Freeman et al., 2012). Generally, for a fetus beyond 32 weeks gestation, a normal or reactive NST consists of two accelerations of the FHR greater than 15 beats above baseline lasting at least 15 seconds occurring in 20 minutes. When the fetus is less than 32 weeks, the immature central nervous system may not respond as vigorously. In these fetuses, a reactive NST consists of two accelerations of greater than 10 beats above baseline lasting at least 10 seconds (L. A. Miller et al., 2017). The NST may continue for 40 minutes or more to account for a fetal sleep cycle.
Vibroacoustic stimulation, using an artificial larynx, may be used to stimulate fetal movement and shorten the test duration (Tan, Smyth, & Wei, 2013). FHR accelerations, in response to fetal scalp stimulation or fetal acoustic stimulation, are predictive of a normal fetal scalp pH (L. A. Miller et al., 2017). A reactive NST may occur without maternal perception of fetal movement (ACOG, 2014; Freeman et al., 2012; L. A. Miller et al., 2017).
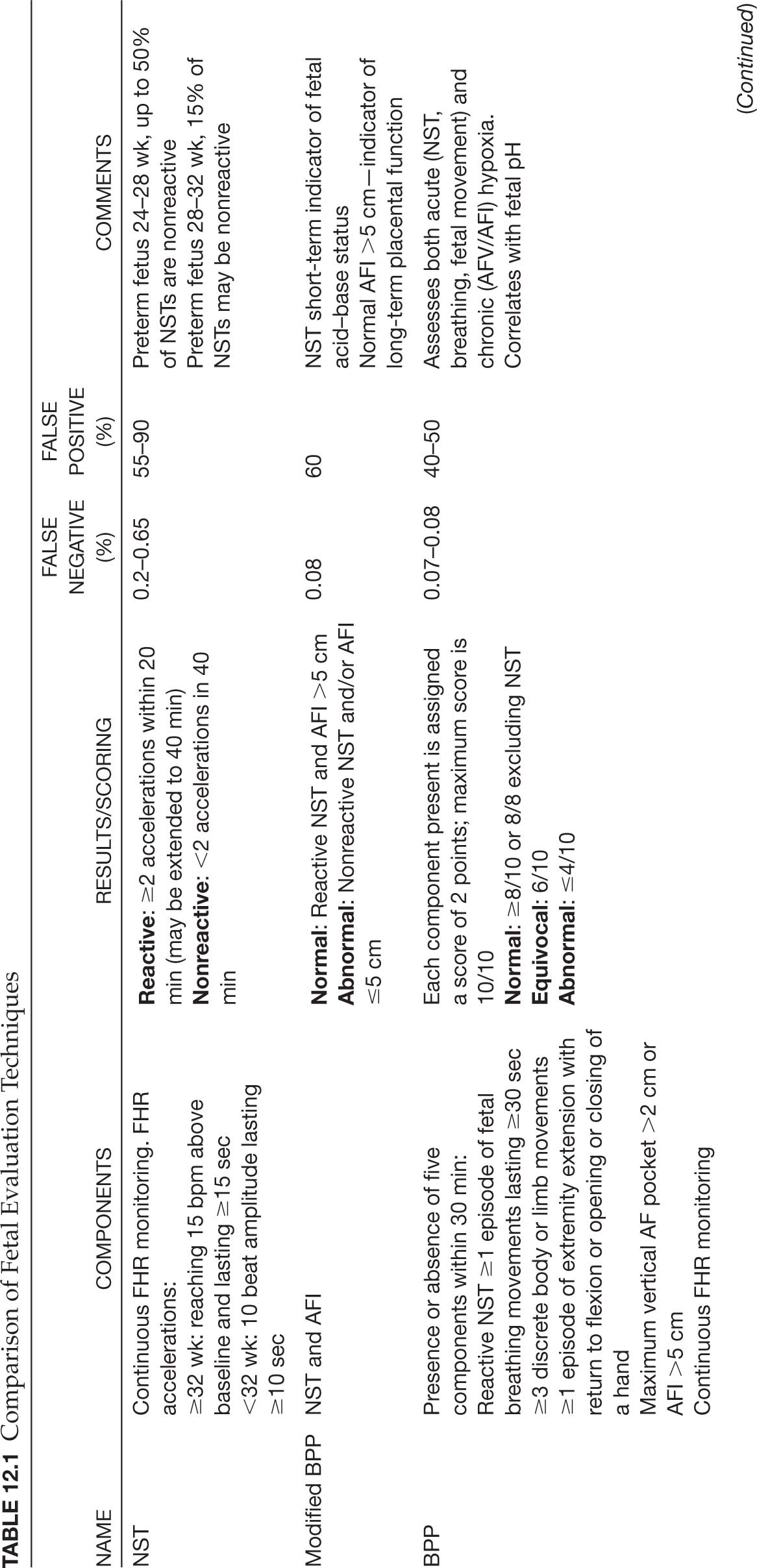
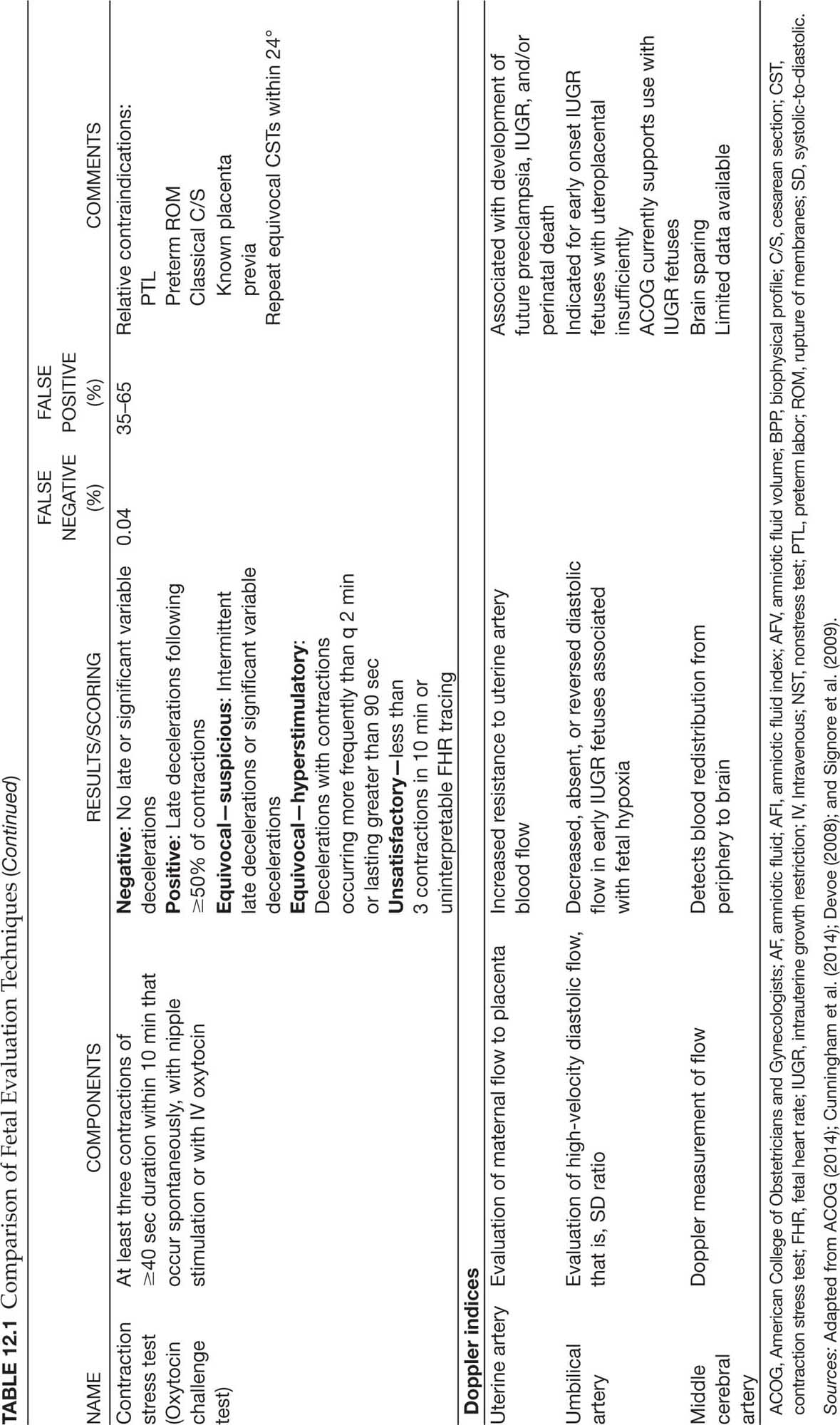
TABLE 12.2 Electronic Fetal Monitoring Standardized Definitions
PATTERN | DEFINITION |
Baseline | Mean FHR rounded to the nearest 5 bpm in 10-min segment excluding accelerations, decelerations, or periods of marked variability Minimum of 2 min of tracing Normal baseline FHR: 110–160 bpm Tachycardia: >160 bpm Bradycardia: <110 bpm |
Baseline variability | Fluctuations in baseline FHR in a 10-min window, peak-to-trough amplitude, and frequency quantified in bpm Absent—range undetectable Minimal—range detectable 5 bpm or less Moderate (normal)—range between 6 and 23 bpm Marked—range >25 bpm |
Accelerations | Abrupt (onset to peak <30 sec) increase in FHR above baseline Peak of acceleration is 15 bpm above baseline and is sustained for ≥15 sec but less than 2 min Before 32 weeks gestation: 10 bpm amplitude for at least 10 sec but less than 2-min duration Prolonged acceleration: >2 min but <10 min if ≥10 min is a baseline change |
Early deceleration | Gradual (onset to nadir >30 sec) decrease and return of FHR associated with a contraction Nadir of deceleration occurs with peak of contraction and returns to baseline with end of contraction |
Late deceleration | Gradual (onset to nadir >30 sec) decrease in FHR below baseline occurring with a contraction “Delayed” timing: Nadir of deceleration occurs after the peak of the contraction and ends after contraction is finished “Repetitive”: Occurs with >50% of uterine contractions |
Variable deceleration | Abrupt (onset to nadir <30 sec) decrease in FHR ≥15 bpm drop below the baseline lasting ≥15 sec, but less than 2 min |
Prolonged deceleration | FHR decrease ≥15 bpm lasting ≥2 min but <10 min; if ≥10 min, it is a baseline change |
Sinusoidal pattern | Smooth, sine-like undulating pattern of FHR baseline with a cycle frequency of 3–5/min lasting for ≥20 min |
Uterine contractions frequency | The number of contractions in a 10-min window averaged over 30 min ≤5 is “normal” >5 is “tachysystole” Management guided by presence or absence of deceleration |
bpm, beats per min; FHR, fetal heart rate.
Sources: Adapted from ACOG (2009, 2010) and D. A. Miller (2010).
An NST is considered nonreactive when two accelerations do not meet the gestational age requirements in 40 minutes (ACOG, 2014). Nonreactive NSTs, along with reactive NSTs with decelerations, warrant additional testing including amniotic fluid (AF) assessment, contraction stress test (CST), or 130biophysical profile (BPP; L. A. Miller et al., 2017). See Figure 12.1 for a sample management algorithm for EFM testing in the obstetric triage setting.
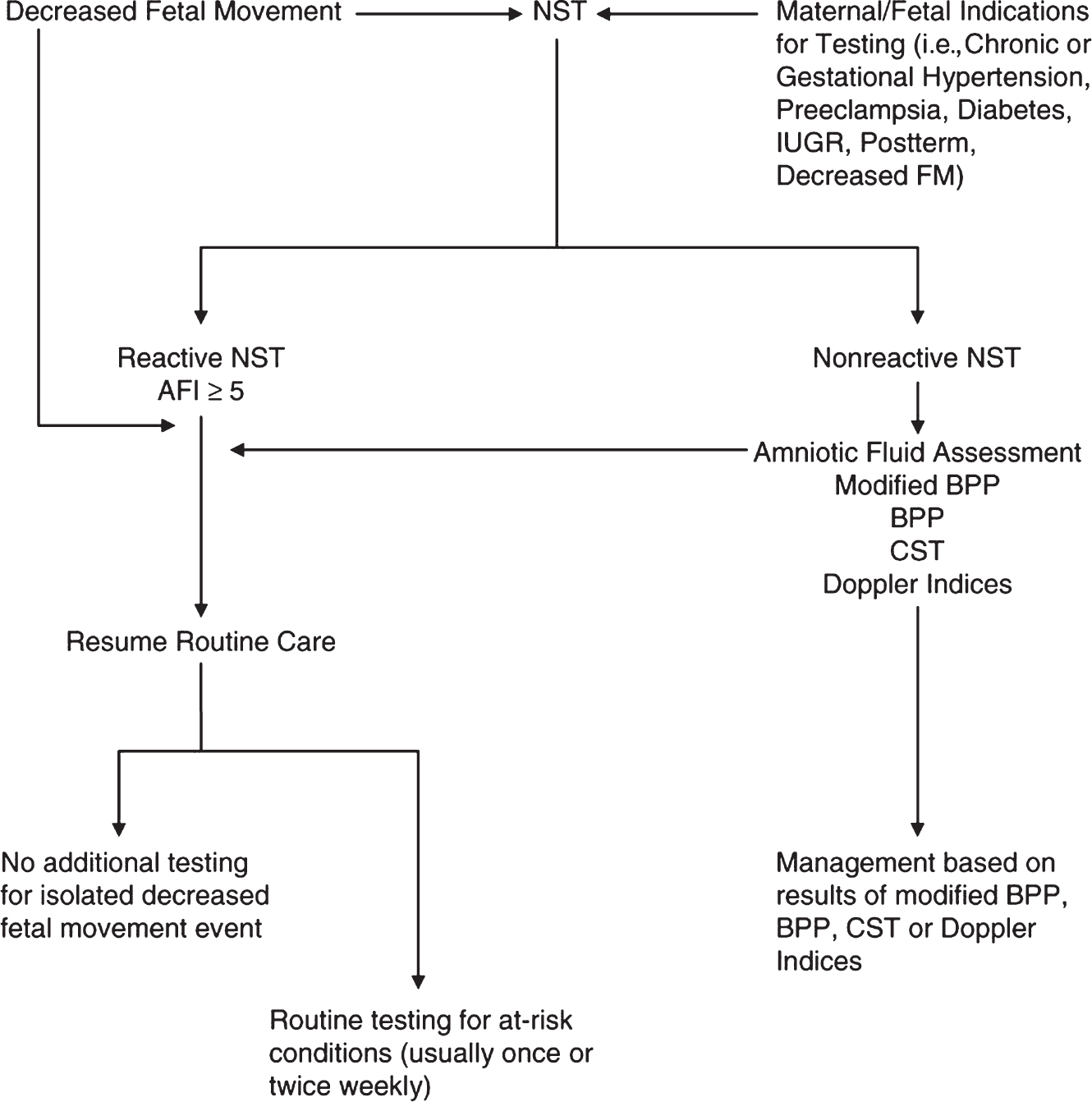
Figure 12.1 Algorithm for electronic fetal monitoring testing
Source: Adapted from L. A. Miller et al. (2017).
AFI, amniotic fluid index; BPP, biophysical profile; CST, contraction stress test; FM, fetal movement; IUGR, intrauterine growth restriction; NST, nonstress test.







Full access? Get Clinical Tree


