CHAPTER 26 Femoral nerve block
Clinical anatomy
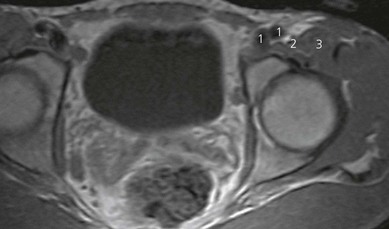
The femoral nerve arises from the ventral rami of the second, third, and fourth lumbar nerves. It descends through the substance of the psoas major, emerging from the muscle at the lower part of its lateral border, and passes down between it and the iliacus muscle, deep to the fascia iliaca (Fig. 26.1). It then passes behind the inguinal ligament to enter the thigh. The nerve lies deep to the fascia lata and fascia iliaca. The fascia iliacus separates it from the vascular bundle containing the femoral artery and vein (Fig. 26.2). It divides into two major branches (anterior and posterior) early in the proximal anterior thigh (Fig. 26.1).

Surface anatomy
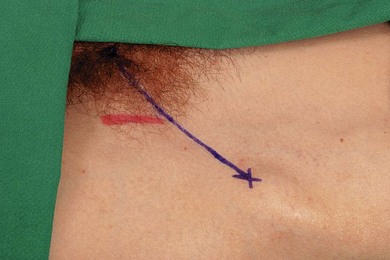
The main landmarks for femoral nerve block are the anterior superior iliac spine, the pubic tubercle, inguinal ligament, inguinal crease, and femoral artery (Fig. 26.3). The pubic tubercle can be palpated three fingers’ breadth from the midline, along the upper border of the pubis. The inguinal ligament is outlined by a line connecting the anterior superior iliac spine and the pubic tubercle.
Sonoanatomy
The femoral nerve is found lateral to the femoral artery in the groin, lying outside the femoral sheath and beneath the fascia lata and iliaca. These fascial layers are seen as hyperechoic lines. Its appearance on ultrasound (Fig. 26.4) is similar to many peripheral nerves, and described as multiple round or oval hypoechoic (dark) areas encircled by hyperechoic (bright) rims. The hypoechoic structures are the nerve fascicles. The femoral nerve may be identified on ultrasound as an oval (95% oval beneath the inguinal ligament) or triangular-shaped structure measuring approximately 3 mm in anteroposterior diameter and 10 mm in mediolateral diameter. Correct transducer angulation is essential for adequate nerve visualization. Femoral nerve anisotropy occurs with transducer angulation of as little as 10° from the vertical. Anisotropy is a property of muscles, nerves, and tendons which relates to the change in ultrasound appearance of the target structure with the scanning angle used. Nerves are best visualized when the ultrasound beam hits them at 90°. In this case, the femoral nerve becomes isoechoic with surrounding structures, and disappears from view, when the transducer is angled 10–13° from the vertical.
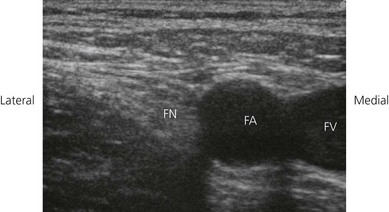
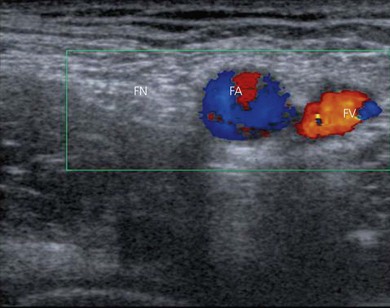
To identify the femoral nerve, the transducer is placed over the femoral vessels on the anterior thigh at 90° to the expected orientation of the nerve and vessels (Fig. 26.5). The vessels may be identified as large round hypoechoic structures, and blood flow may be demonstrated using colorflow Doppler (Fig. 26.6). The femoral nerve is then visualized a variable distance lateral to the femoral artery.

Technique
Landmark-based approach
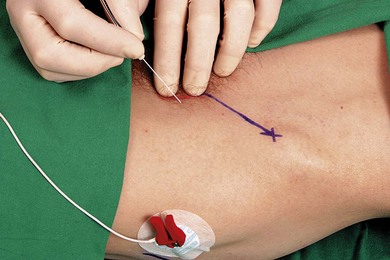
The patient is placed in the supine position with the operator standing on the side to be blocked, at the level of the patient’s thigh. The needle insertion point is infiltrated with local anesthetic using a 25-G needle. A 50-mm 21-G insulated needle is oriented in a 45° cephalad and posterior orientation lateral to the palpated femoral artery at the inguinal crease (Fig. 26.7). The stimulating current is set at 1.0 mA, 2 Hz, and 0.1 ms.
< div class='tao-gold-member'>







Full access? Get Clinical Tree


