Facet Joint Procedures: Facet Joint Injections, Medial Branch Blocks, and Radiofrequency Ablation of the Medial Branches of the Spinal Nerve Roots
The facet joint is a synovial-lined joint that links two vertebral bodies posteriorly (Fig. 20-1).
In the lumbar spine, the facet joint is formed by the articulation of the inferior articulating process of one lumbar vertebra with the superior articular process of the next vertebra. Facet joints allow the spine to flex, extend, and rotate. Wear and tear caused by our body movement over time can cause these joints to become arthritic and painful (Fig. 20-2). When our intervertebral discs lose height as part of the normal aging
process, up to 70% of the compressive force usually applied to the discs may be transferred to the facet joints.1 The most commonly affected are the lower cervical (C4/C5 and C5/C6) and the lower lumbar (L3/L4, L4/L5, and L5/S1) facet joints. The lumbar facet joints are particularly vulnerable because the distribution of axial weight along the spine is greatest at these levels and because this is where the greatest range of motion in the spine occurs. Pain from a facet joint is transmitted to the brain via the medial branch of the posterior division of the spinal nerve roots. For each facet joint there is a medial branch that innervates the superior aspect of the facet joint and one that innervates the inferior aspect (Fig. 20-3).
process, up to 70% of the compressive force usually applied to the discs may be transferred to the facet joints.1 The most commonly affected are the lower cervical (C4/C5 and C5/C6) and the lower lumbar (L3/L4, L4/L5, and L5/S1) facet joints. The lumbar facet joints are particularly vulnerable because the distribution of axial weight along the spine is greatest at these levels and because this is where the greatest range of motion in the spine occurs. Pain from a facet joint is transmitted to the brain via the medial branch of the posterior division of the spinal nerve roots. For each facet joint there is a medial branch that innervates the superior aspect of the facet joint and one that innervates the inferior aspect (Fig. 20-3).
 Figure 20-1 Lumbar facet joints connect the posterior aspect of the spine, they allow the spine to flex, extend, and rotate. Facet joints are formed by a inferior and superior articulating processes. |
 Figure 20-2 Arthritic lumbar facet joints. |
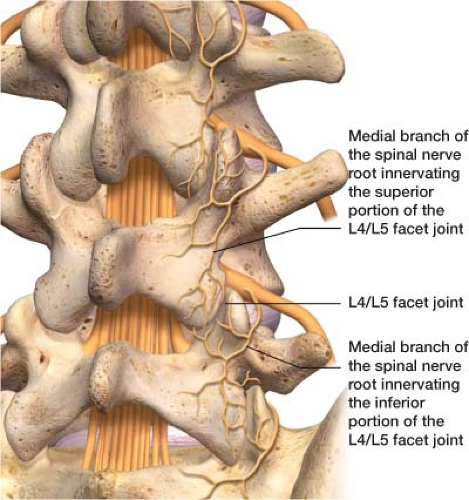 Figure 20-3 The L4/L5 facet joint innervated by the medial branch of the spinal nerve above and below it. Pain emanating from a facet joint is transmitted to the brain via these medial branches. |
Facet joint pain is axial in nature rather than radicular. Radicular pain runs from the lower back to the foot or in the cervical spine from the neck to the hands. Facet pain is often described as deep and achy. The pain is focal over the area of arthropathy. Deep palpation over the facet joint may elicit pain. Some doctors have patients extend the lower back and rotate toward the side of pain as a mechanism to stress the facet joints. From a mechanical point of view, extension and extension rotation stress facet joints but probably stress disc and ligaments more.2
The diagnosis of facet joint-mediated pain is obtained by response to a diagnostic block. If based on the history and examination you feel that pain seems to be coming from facet joint arthropathy, it is reasonable to arrange a block for the patient. The facet joints are paired joints—a facet joint on the left and right sides of the spine links two vertebral bodies. Your patient may have pain over the bottom two facet joints—L4/L5 and L5/S1—on the right only (Fig. 20-4). In this case, you would do a unilateral block of the L4/L5 and L5/S1 facet joints on the right. The diagnosis of
facet-mediated pain is clinical and not radiographic. The degree of degeneration identified on radiologic evaluation does not correlate with the severity of facet joint pain. However, if the patient has a normal magnetic resonance imaging (MRI) or computed tomography (CT) scan of their spine it is unlikely their pain is facet joint mediated. There are two ways to perform a diagnostic block: (1) The joint itself is injected with a local anesthetic or (2) anesthetize the medial branches of the spinal nerve roots that innervate a particular facet joint. If the facet joint is the pain generator, both the intra-articular (in the joint) or medial branch diagnostic blocks will temporarily relieve the pain produced from the facet joint. Typically, patients receive a pain diary to fill out before the injection and immediately after the procedure. The diary tracks the visual analog pain score over time. The block is considered positive if it relieves pain in the area from which pain could be expected to be blocked. If the pain is not relieved, a new hypothesis regarding the source of the patient’s pain needs to be developed.
facet-mediated pain is clinical and not radiographic. The degree of degeneration identified on radiologic evaluation does not correlate with the severity of facet joint pain. However, if the patient has a normal magnetic resonance imaging (MRI) or computed tomography (CT) scan of their spine it is unlikely their pain is facet joint mediated. There are two ways to perform a diagnostic block: (1) The joint itself is injected with a local anesthetic or (2) anesthetize the medial branches of the spinal nerve roots that innervate a particular facet joint. If the facet joint is the pain generator, both the intra-articular (in the joint) or medial branch diagnostic blocks will temporarily relieve the pain produced from the facet joint. Typically, patients receive a pain diary to fill out before the injection and immediately after the procedure. The diary tracks the visual analog pain score over time. The block is considered positive if it relieves pain in the area from which pain could be expected to be blocked. If the pain is not relieved, a new hypothesis regarding the source of the patient’s pain needs to be developed.
 Figure 20-4 Painful L4/L5 and L5/S1 facet joints on the right. The left L4/S5 and L5/S1 facet joints are without arthropathy. |
It is important to remember that patients may have more than one source of back pain. As wear and tear develops in the spine over the years, there is increased destruction of the facet joints, intervertebral discs, and nerve roots. For example, patients can have facet joint pain and lumbar radiculopathy. A diagnostic injection can help you determine the facet joint generator component of the pain.
If the patient and the patient’s pain diary indicate a positive response, the patient undergoes a second diagnostic injection to ensure that the first response was not a false-positive result. Controlled studies have shown that single blocks carry a false-positive rate of 38%.3 To confirm that the results are repeatable, it is necessary to perform second injection.
If you have targeted which facet joints are the pain generator, and the patient has had two positive responses to diagnostic injections, the next step is to use radiofrequency (RF) ablation for a more permanent block. RF ablation uses a very controlled source of heat to destroy the medial branches that innervate a particular facet joint. The theory is that even though the painful facet joint remains unchanged (unless surgery has been performed), the medial branches of the spinal nerve roots can no longer send painful impulses to the posterior division of the spinal nerve and then up to the brain if it is ablated. This ablation process results in neutralization of the painful facet joints but does not alter the structural integrity of the joint. Pathologic pain is being eliminated—the patient will still have the awareness to properly protect the spine. Typically, the effects last 6 to 18 months because the nerve may regenerate. In a selected group of patients using strict criteria and proper techniques, 87% of patients had a 60% pain reduction at 1 year.4 If the symptoms return, a repeat procedure is done. There is no cumulative risk to repeating the RF procedure.
There are two common questions regarding facet joint procedures: Diagnostic injection versus diagnostic therapeutic injection and facet joint injections versus medial branch blocks. The following sections discuss these issues.
When to use
Diagnostic Injection Versus Diagnostic Therapeutic Injection
The purpose of a diagnostic injection is to identify whether a facet joint or joints are the pain generator. This is accomplished by using a local anesthetic. In academic centers, patients receive two injections. A local anesthetic will be used with the first diagnostic injection and if the patient has pain relief, the second diagnostic injection again using a local anesthetic is performed.
In some academic centers and most private practices, patients often choose to have an injection that can be both diagnostic and therapeutic rather than one that is simply diagnostic—for financial and physiologic reasons. Injection of a steroid–local anesthetic mixture into the facet joint or on the medial branch of the spinal nerve roots is diagnostic, but it may also reduce inflammation, providing a therapeutic effect. Young people with facet pain caused by minor trauma or strain may experience permanent pain relief. Older people with facet pain caused by osteoarthritis may have months of pain relief.
Facet Joint Injections Versus Medial Branch Blocks
In clinical practice, some physicians use intra-articular facet joint injections, whereas others use medial branch blocks. The rationale for using intra-articular injections is that they can be both diagnostic and therapeutic. Injecting steroids into any joint—including painful facet joints—can provide longer-lasting pain relief, thus indicating that the pain originated in the facet joint. The rationale for not using intra-articular facet joint injections as a diagnostic block is that they lack a direct valid subsequent treatment. The next step to a positive diagnostic facet joint block is RF ablation of the medial branches of the respective spinal nerve roots branches not the joint itself. The rationale for not using medial branch blocks as a therapeutic tool rather than strictly a diagnostic injection is if a combination of a steroid and a local anesthetic is used as the
therapeutic agent and the steroid is injected near the joint but not into it, the block may not provide long-lasting pain relief.
therapeutic agent and the steroid is injected near the joint but not into it, the block may not provide long-lasting pain relief.
How to Perform the Procedure
This section discusses the basics of facet joint injections, medial branch blocks, and RF ablation of the medial branches of spinal nerve roots. For all treatments, it is necessary to explain the procedure to the patient completely, answer all questions, and obtain informed consent. On arrival in the fluoroscopy suite the patient lies down on the fluoroscopic table in the prone position (face down). A pillow placed under the abdomen makes the lumbar facet joints more accessible. Facet joint procedures are done under fluoroscopic guidance (live x-ray) for accuracy and safety. A “time out” is performed prior to the procedure including verbal confirmation of correct patient, procedure and procedural site. Noninvasive hemodynamic monitors and pulse oximetry are placed. Finally, the procedure requires that the skin is prepped with Betadine and drapes are placed over the area in standard sterile fashion.
Related posts:







Full access? Get Clinical Tree


