A. Cervical Facet Block
 Patient Position:
Patient Position: Supine, for medial branch block.
 Indications:
Indications: Cervical facet syndromes as seen with sudden stop of vehicle (whiplash), athletic or occupational injury, sleeping with the neck in odd (twisted) positions, and degenerative changes such as those seen in osteophyte formation or joint capsule hypertrophy.
 Needle:
Needle: 22-gauge, 88-mm spinal needle.
 Medication/Volume:
Medication/Volume: 0.1 to 0.2 mL (<0.5 mL) radio-opaque dye (Isovue-M 200, Bracco Diagnostics, Princeton, NJ), 0.5 to 1.0 mL 0.5% bupivacaine plus 40 mg triamcinolone acetate.
 Anatomic Landmarks:
Anatomic Landmarks: Seven cervical vertebrae with two facet joints at each level, synovial in type. At this level, the facets are posterior to the transverse process and are formed by the superior articular facet of the lower vertebra articulating with the inferior articular facet of the upper vertebra. The joint surfaces are midway between the coronal and axial planes. The capsule of the facet joint is tough and fibrous posteriorly, and is in direct contact with the ligamentum flavum on its anteromedial aspect, adjacent to the neural foramen and nerve root. Dual level innervation is from the segmental nerve at its vertebral level and also the nerve at the level caudad to it.
 Approach and Technique:
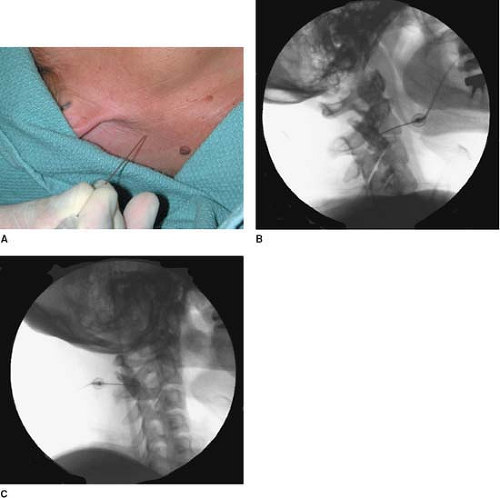
Approach and Technique: The cervical region is prepared and draped using sterile techniques. Under fluoroscopic guidance, the cephalocaudad vertebral level of the facet to be blocked is marked
(Fig. 64-1A). The mediolateral position of the facet joint is also visualized by rotating the fluoroscope to produce an oblique image of the cervical spine. After negative
aspiration of blood and cerebrospinal fluid (CSF), needle placement is confirmed with an injection of radiocontrast material. This is then followed with local anesthetic and steroid.
For medial branch blocks (C3-7), the patient is positioned supine with the side to be blocked uppermost. A 20° to 30° oblique view is obtained by rotating the fluoroscope to visualize the foramina (in order to avoid them) and before proceeding with the injection.
Figure 64-1B presents the lateral view (with dye) and
Figure 64-1C presents the oblique view (with dye).
Only gold members can continue reading.
Log In or
Register to continue
Related

Full access? Get Clinical Tree