![]() For repair of a partial or complete tendon injury
For repair of a partial or complete tendon injury
![]() Partial laceration of the extensor tendons proximal to the metacarpophalangeal (MCP) joint may or may not require repair; those at or distal to the MCP joint level must be repaired
Partial laceration of the extensor tendons proximal to the metacarpophalangeal (MCP) joint may or may not require repair; those at or distal to the MCP joint level must be repaired
CONTRAINDICATIONS
![]() Delayed closure and/or referral to a hand specialist or orthopedic surgeon may be more appropriate in the following circumstances:
Delayed closure and/or referral to a hand specialist or orthopedic surgeon may be more appropriate in the following circumstances:
![]() Severe contamination or acute infection
Severe contamination or acute infection
![]() Injuries due to human teeth (clenched fist injury or “fight bite”)
Injuries due to human teeth (clenched fist injury or “fight bite”)
![]() Delayed presentation of injury
Delayed presentation of injury
![]() Extensive injury requiring prolonged use of tourniquet (longer than 20–30 minutes)
Extensive injury requiring prolonged use of tourniquet (longer than 20–30 minutes)
![]() Penetration of laceration into a joint capsule
Penetration of laceration into a joint capsule
![]() These cases may be taken to the operating room for surgical exploration, irrigation, and intravenous (IV) antibiotics
These cases may be taken to the operating room for surgical exploration, irrigation, and intravenous (IV) antibiotics
RISKS/CONSENT ISSUES
![]() Pain
Pain
![]() Bleeding
Bleeding
![]() Infection (theoretical risk of iatrogenic infection)
Infection (theoretical risk of iatrogenic infection)
![]() Risk of injuring other structures—tendons, vessels, nerves
Risk of injuring other structures—tendons, vessels, nerves
![]() Laceration may need to be extended to allow adequate exploration or access to the surgical field
Laceration may need to be extended to allow adequate exploration or access to the surgical field
![]() General Basic Steps
General Basic Steps
![]() Patient preparation (ring removal, tourniquet, irrigation)
Patient preparation (ring removal, tourniquet, irrigation)
![]() Local anesthesia or nerve block
Local anesthesia or nerve block
![]() Thorough wound evaluation
Thorough wound evaluation
![]() Tendon repair
Tendon repair
![]() Apply appropriate splint
Apply appropriate splint
LANDMARKS
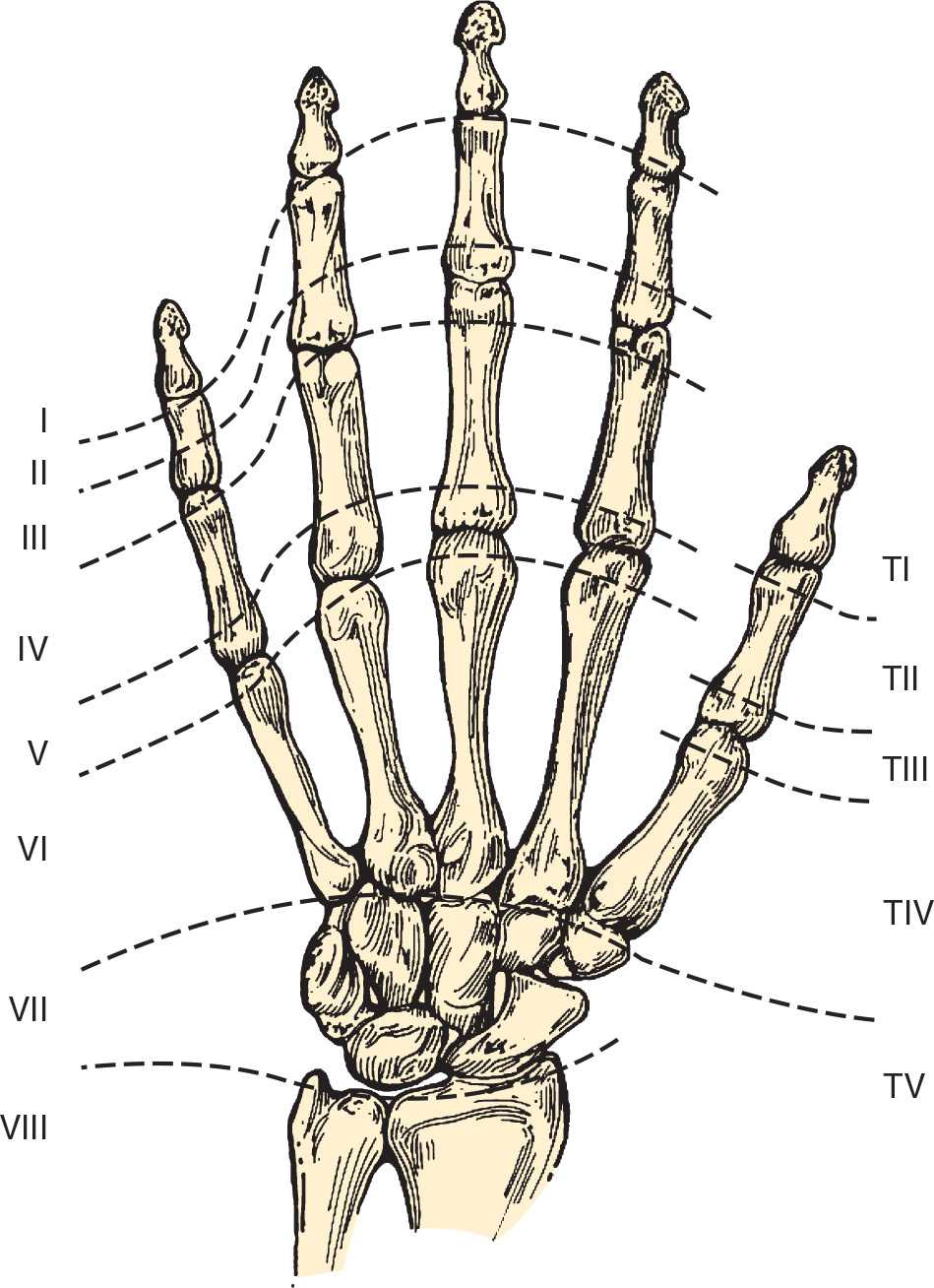
The anatomic location of open extensor tendon injuries in the wrist or hand drives treatment decisions and emergency department (ED) management. The Verdan classification system divides the hand and wrist into eight zones (TABLE 51.1 and FIGURE 51.1), which helps determine if tendon repair should be attempted in the ED.
TECHNIQUE
![]() Preparation
Preparation
![]() Remove all rings immediately!
Remove all rings immediately!
![]() Radiographs, as indicated, should be employed to assess for associated fracture, foreign body, or joint space disruption
Radiographs, as indicated, should be employed to assess for associated fracture, foreign body, or joint space disruption
![]() Place the patient in a comfortable position, preferably supine, with the injury site easily accessible
Place the patient in a comfortable position, preferably supine, with the injury site easily accessible
![]() Obtain proper lighting to optimize wound exploration, which should include thorough assessment for tendon injury and foreign bodies
Obtain proper lighting to optimize wound exploration, which should include thorough assessment for tendon injury and foreign bodies
![]() Sterile technique should be employed
Sterile technique should be employed
![]() Adequate anesthesia should be administered once the initial neurovascular examination is complete. Lidocaine 1% to 2% with epinephrine can be used in the hand except in areas supplied by end arteries. Local infiltration or an appropriate nerve block can be used.
Adequate anesthesia should be administered once the initial neurovascular examination is complete. Lidocaine 1% to 2% with epinephrine can be used in the hand except in areas supplied by end arteries. Local infiltration or an appropriate nerve block can be used.
![]() The wound should be thoroughly irrigated and free of contamination. Debridement of grossly contaminated tissue may be necessary.
The wound should be thoroughly irrigated and free of contamination. Debridement of grossly contaminated tissue may be necessary.
![]() Good hemostasis is critical to wound exploration and tendon repair
Good hemostasis is critical to wound exploration and tendon repair
![]() Elevate the arm for 1 minute to facilitate drainage of blood before applying a tourniquet
Elevate the arm for 1 minute to facilitate drainage of blood before applying a tourniquet
![]() Inflate a blood pressure cuff to 260 to 280 mm Hg and clamp the cuff tubes to avoid air leak, or use commercial tourniquets for arm or finger
Inflate a blood pressure cuff to 260 to 280 mm Hg and clamp the cuff tubes to avoid air leak, or use commercial tourniquets for arm or finger
![]() Apply the tourniquet for no longer than 20 minutes
Apply the tourniquet for no longer than 20 minutes
THE VERDAN CLASSIFICATION SYSTEM |
Zone | Finger | Thumb |
I | DIP joint | IP joint |
II | Middle phalanx | Proximal phalanx |
III | PIP joint | MCP joint |
IV | Proximal phalanx | Metacarpal |
V | MCP joint | CMC joint |
VI | Metacarpals |
|
VII | Carpals |
|
VIII | Proximal wrist and distal forearm |
|
DIP, distal interphalangeal; IP, interphalangeal; PIP, proximal interphalangeal; MCP, metacarpophalangeal; CMC, carpometacarpal. | ||

Full access? Get Clinical Tree


