Chapter 27 Esophageal-Tracheal Double-Lumen Airways
The Combitube and EasyTube
I Combitube
A Use of the Endotracheal Tube for Intubation and Ventilation
Rapid establishment of a patent airway to facilitate adequate ventilation during cardiopulmonary resuscitation (CPR) is the primary task of the rescuer. Mouth-to-mouth ventilation carries the disadvantages of possible gastric insufflation and the danger of aspiration. Endotracheal intubation remains the gold standard in airway maintenance, but this skill is acquired only after intensive training and requires constant practice. The people performing resuscitation procedures often are untrained in intubation, which is sometimes difficult or impossible even for skilled personnel.1 It requires good exposure of the patient’s airway, a skilled endoscopist, and equipment or facilities for intubation. Because the main objectives of airway management are ventilation and oxygenation, the need arises for a simple and efficient alternative to endotracheal intubation.2
B Use of the Esophageal Obturator Airway as an Alternative Airway Adjunct
The esophageal obturator airway was constructed by Don Michael and colleagues as an alternative to using the endotracheal tube during emergency intubation.3 The esophageal obturator airway is a 34-cm-long tube with a balloon at its distal tip (Fig. 27-1). The balloon should lie below the level of the tracheal bifurcation after insertion. The distal end is blocked. Proximal to the balloon, there are 16 holes that are positioned in the region of the hypopharynx after positioning the airway. At the proximal end, a face mask is connected to the airway, sealing the mouth and nose during ventilation.
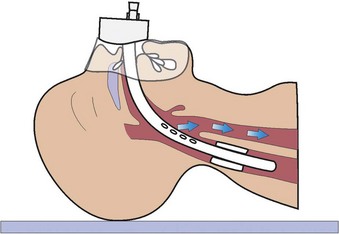
The esophageal obturator airway is inserted by first grasping the back of the patient’s tongue and the lower jaw with the thumb and index finger and then guiding the airway gently into the esophagus. The distal balloon is inflated to occlude the esophagus while the mask is pressed against the patient’s face. Air enters the proximal end and then enters the hypopharynx through perforations because the distal end is blocked. From there, air is forced over the opened glottis into the trachea because the mouth and nose are sealed by the mask and the esophagus by the balloon (see Fig. 27-1).
1 Testing and Trials of the Esophageal Obturator Airway
Subsequent physiologic testing and field trials of the esophageal obturator airway have been performed. Schofferman and colleagues evaluated the airway in 18 patients suffering from cardiac arrest,4 in whom resuscitation was performed by paramedics. Arterial blood gas analysis was obtained during ventilation with the esophageal obturator airway and subsequently with the endotracheal tube (ETT). There was little or no improvement in oxygenation after endotracheal intubation, implying that failure to oxygenate some patients did not result from the esophageal obturator airway.
Shea and associates compared two similar groups of patients during cardiopulmonary arrest with ventricular fibrillation5; 296 patients were intubated with an ETT or esophageal obturator airway. Survival rates and neurologic sequelae of survivors showed no statistically significant difference for the two groups. Hammargren and colleagues compared both devices after standardizing the method of oxygen delivery and ensuring true sampling of arterial blood.6 In 48 victims who had prehospital cardiac arrest, blood gases were sampled during ventilation with the esophageal obturator airway and subsequent ventilation with the ETT. There was no statistically significant difference between the two devices for the PaO2 and PaCO2 values. The investigators concluded that the esophageal obturator airway was an effective means of airway management, with the ventilation achieved equal to that of an ETT. Nevertheless, it soon became apparent from studies in the controlled environment of the operating room that considerable technical difficulties were associated with the esophageal obturator airway.7
2 Disadvantages of the Esophageal Obturator Airway
1. There are significant difficulties in obtaining a tight face mask seal and maintaining the seal during transportation. Effective use requires at least two hands to seal the mask. Obtaining an adequate mask fit is particularly difficult in edentulous or bearded patients.6,7
2. Inadvertent or unrecognized tracheal intubation may occur.8 The patient’s airway is completely obstructed, and attempts at repositioning are usually unsuccessful.
3. Esophageal or gastric ruptures have been reported.9–12 Ruptures of the esophagus or the stomach may be due to the length of the esophageal obturator airway. Because many cardiac arrest patients exhibit left atrial dilatation with subsequent lateral deviation of the lower half of the esophagus, the esophageal obturator airway may be forced in a left lateral direction in addition to the curved sagittal direction, which can lead to ruptures.
C Development of the Combitube Esophageal-Tracheal Double-Lumen Airway
The previously described disadvantages and the idea that both tracheal and esophageal intubation allow ventilation and oxygenation led to the development of the Combitube. It was devised by Michael Frass in cooperation with Reinhard Frenzer and Jonas Zahler in Mödling and Vienna, Austria.13–17
The Combitube design was intended to deal effectively with the problem of managing the airway with the greatest success possible. Studies in large populations demonstrate that the Combitube provides a much better chance of ventilation and oxygenation than other devices18–21 by isolating and protecting the airway from digestive regurgitation and aspiration.22 The Combitube can be used when airway management is difficult independent of the cause, such as anatomic factors, the patient’s position with respect to the operator, space and illumination restrictions, and presence of a full stomach. The Combitube does not need special equipment, energy, or complex techniques to be properly used. Because the Combitube is available in only two sizes (37 and 41 F), no time is lost in selecting the proper size among many alternatives.
D Technical Description
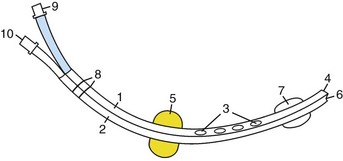
The Esophageal Tracheal Combitube (Combitube; Tyco Healthcare, Mansfield, MA) is a device for emergency intubation that combines the functions of an esophageal obturator airway and a conventional ETT (Fig. 27-2). The Combitube is a double-cuff and double-lumen tube (Fig. 27-3). The oropharyngeal balloon is located at the middle portion of the tube and the tracheoesophageal cuff is located at the distal end.23 The lumens are separated by a partition wall. Proximally, both lumens are opened and linked by short tubes with universal connectors. Distally, the pharyngeal lumen is blocked and has eight perforations at the level between the cuffs, and the tracheoesophageal lumen is open. This design allows ventilation when the Combitube is positioned in the esophagus through the perforations of the pharyngeal lumen and in the trachea through the opened distal end of the tracheoesophageal lumen. The pharyngeal balloon seals the oral and nasal cavities after inflation. Printed ring marks proximal to the oropharyngeal balloon indicate the limit of insertion.

The 37-F Small Adult (SA) Combitube may be used in patients 4 to 6.5 ft tall.18,24,25 The 41-F model is used in patients taller than 6 ft (with some overlap with the SA model). The 37-F SA Combitube usually is the preferred model because it works well in patients up to 6.5 ft tall.
E Insertion Techniques
1 Conventional Technique
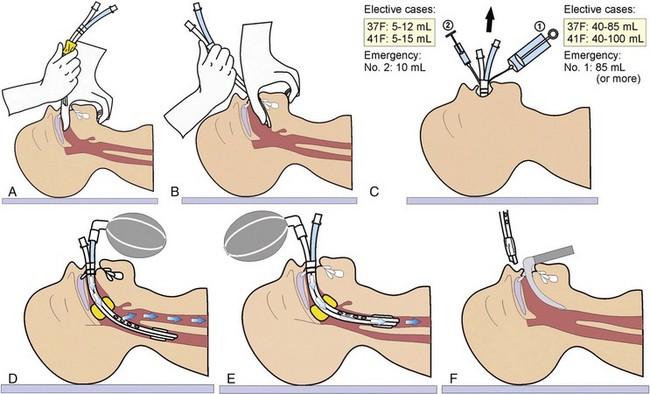
With the operator behind the patient’s head, the lower jaw and tongue are lifted by the thumb and index finger. The tongue is pressed forward by the thumb, and the tube is inserted in a curved downward movement until the printed ring marks lie between the teeth or the alveolar ridges in edentulous patients (Fig. 27-4A). The insertion should be performed along the tongue to avoid potential damage of the posterior pharyngeal mucosa. Sometimes, a rocking motion may alleviate problems encountered with insertion. Next, the oropharyngeal balloon is inflated with up to 85 mL of air for the 37-F SA Combitube (or up to 100 mL for the 41-F Combitube) through port no. 1 with the blue pilot balloon using the large syringe with the blue color code (see Fig. 27-4B). When the minimal-volume technique is used, enough air is added to inflate the balloon and obtain a seal (see “General Anesthesia”), or a cuff pressure gauge may be used to achieve a seal of 60 mm Hg. If sufficient sealing of the mouth and nose cannot be accomplished, the oropharyngeal balloon may be filled with an additional 50 mL of air, up to a total amount of 150 mL.26
During inflation, the tube may move slightly out of the patient’s mouth because of the self-positioning properties of the balloon. A useful sign indicating malposition due to insufficient insertion is that the inflated pharyngeal balloon can be seen when looking into the patient’s mouth (Fig. 27-5). If this occurs, the pharyngeal balloon should be deflated, and the tip’s position should be reevaluated. The Combitube may become kinked during placement, and reinsertion may be necessary. The anatomic relationships of the oropharyngeal balloon have been demonstrated radiologically.26 The balloon protrudes in an oral direction after overinflation so that it does not close the epiglottis. Figure 27-6 shows a cross-sectional magnetic resonance imaging (MRI) view of the Combitube in the esophageal position. It displays anterior movement of the larynx, a situation that can often be observed clinically. Knowledge of this may facilitate subsequent location of the larynx for endotracheal intubation.

Figure 27-5 Seeing the inflated oropharyngeal balloon in the patient’s mouth indicates malposition of the Combitube.

Figure 27-6 Cross-sectional MRI view of a patient intubated with Combitube in the esophageal position.
(Courtesy of B. Panning, MD, Department of Anesthesiology, and C. Ehrenheim, MD, Department of Nuclear Medicine and Special Biophysics, Hannover School of Medicine, Hannover, Germany.)
The distal balloon is then inflated with 10 mL of air through port no. 2 with the white pilot balloon and using the small syringe.27 With blind insertion, there is a high probability that the tube will be placed into the esophagus. Test ventilation is recommended through the longer, blue no. 1 tube leading to the esophageal lumen (see Fig. 27-4C). Air passes into the pharynx and then through the glottis into the trachea because the mouth, nose, and esophagus are blocked by the balloons. Auscultation of breath sounds in the absence of gastric insufflation confirms adequate ventilation when the Combitube is in the esophagus. Ventilation is then continued through this lumen. In this position, the Combitube allows closed suctioning and active decompression of the stomach.28 Closed suctioning provides the advantage of reduced cross contamination between the bronchial system and gastric juices.29 Gastric contents can be suctioned through the unused tracheoesophageal lumen with the help of a small suction catheter (10 or 12 F) included in the kit.
The most common cause of failed ventilation through the blue connector is a tracheal position of the distal tip (see Fig. 27-4D). Without changing the position of the Combitube, ventilation is changed to the shorter, transparent no. 2 tube leading to the tracheoesophageal lumen, and the position is again confirmed by auscultation. Ventilation is then carried out through the tracheoesophageal lumen directly into the trachea. The oropharyngeal balloon may be deflated in case of regurgitation to allow suctioning with a conventional catheter. Otherwise, the balloon should remain inflated to stabilize the Combitube.
If no breath sounds are heard over the lungs or a capnographic curve is absent while ventilating through the blue connector, the second most common cause is that the Combitube has been inserted too deeply, and the oropharyngeal balloon lies just opposite the laryngeal aperture and occludes the airway.30 In this situation, both balloons should be deflated and the Combitube pulled back about 2 to 3 cm out of the patient’s mouth and then fixed in this position.
The third most common cause of failed ventilation is a phenomenon (e.g., laryngospasm, bronchospasm, pulmonary edema) leading to high airway pressure. In this situation, cause should be identified and treated. Unlike other airway devices, the Combitube allows ventilation against high airway pressure, and administration of inhaled bronchodilators28,31 and proper treatment of the spastic phenomenon can be started immediately after full inflation of the balloon to ensure high-pressure ventilation.
An investigation by Wafai and coworkers was designed to test the reliability of the self-inflating bulb in identifying the location of the Combitube and facilitating its proper position in anesthetized patients.32 In group 1 (n = 26), the Combitube was introduced blindly. In group 2 (n = 20), the tube was placed in the trachea (8 patients) or once in the trachea and once in the esophagus randomly (12 patients) under direct vision rigid laryngoscopy by the anesthesiologist performing the intubation. In both groups, the efficacy of the self-inflating bulb in identifying the location of the Combitube was tested by a second blinded anesthesiologist. In group 1, blind insertion of the Combitube resulted in esophageal placement in all patients, and in each case, it was correctly identified. The second anesthesiologist reported no reinflation when the compressed self-inflating bulb was connected to the distal lumen. When the compressed self-inflating bulb was connected to the proximal lumen, instantaneous reinflation was observed in 23 patients, delayed reinflation (2 to 4 seconds) in 2, and no reinflation (>4 seconds) in 1. Instantaneous reinflation occurred in these three patients after repositioning the Combitube. In group 2, the second anesthesiologist correctly identified the location of the Combitube in all cases. The results confirm previous findings that blind introduction of the Combitube leads to esophageal placement and yields adequate ventilation. The self-inflating bulb can quickly identify the location of the Combitube and facilitate its positioning with the use of a simple algorithm. This can be important if the Combitube is used in a patient whose lungs cannot be ventilated by mask and whose trachea cannot be intubated.
2 Alternative Insertion Technique
Another way of inserting the Combitube has been described by Urtubia and colleagues.33 This insertion technique (Fig. 27-7A and B) consists of grasping the upper teeth or the upper alveolar ridge with the index finger while pushing the chin with the middle finger. To avoid contact of the tip of the Combitube with the posterior oropharyngeal wall, Urtubia recommends keeping the Combitube bent as long as possible before blind insertion.33 Similarly, Urtubia and associates describe a modification of the Lipp maneuver for blind insertion of the Combitube.34
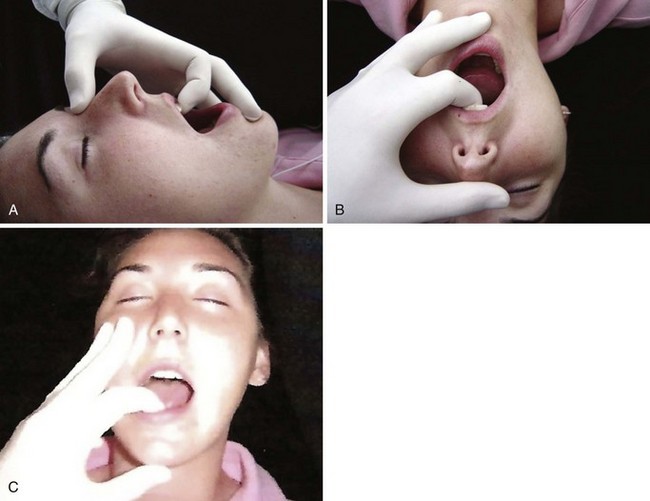
Figure 27-7 A and B, New insertion technique as described by Urtubia and coworkers.33 C, Alternative insertion technique.
(Courtesy of Carin Hagberg, MD, Houston, TX.)
For patients in sitting and prone positions or when the operator is facing the patient, a similar technique can be useful. The index finger grasps the lower teeth or alveolar ridge while the middle finger pushes the cheek (see Fig. 27-7C). The enlarged interincisor distance allows easier insertion of the Combitube, especially in partially edentulous patients and in patients with a limited oral opening (Fig. 27-8A and B). As with the original technique, it does not require any cervical movement, which makes it suitable for patients with cervical spine trauma.

The Combitube may be inserted blindly or with the aid of a laryngoscope. Use of a laryngoscope is recommended during the initial training period when endotracheal intubation using laryngoscopy fails (i.e., insert the Combitube with the laryngoscope still in place) and when blind insertion of the Combitube fails.28
F Indications, Advantages, and Complications
1 Out-of-Hospital Emergency Intubation
The Combitube is especially suitable for emergency intubation in and out of the hospital when endotracheal intubation is not immediately possible. It may be used in the following three situations. First, in patients with difficult anatomy (e.g., bull neck, lockjaw, small mouth opening), the Combitube can be inserted in those with an interincisor distance (i.e., oral aperture) as small as 15 mm.35 Second, the Combitube can be inserted in difficult spatial circumstances, such as limited access to a patient’s head when the patient lies on the floor in a small room, when the patient is lying with his head close to the wall in the general ward or in the intensive care unit (ICU) with many lines at the side impeding quick access to the head, or when a patient is trapped in a car after an accident. Third, the Combitube can be inserted despite challenging illumination, such as bright light, massive bleeding, or regurgitation that can inhibit direct laryngoscopy. The Combitube prevents aspiration, which may occur with repeated suction maneuvers or vomiting.22,24,36
2 Elective and Emergency Surgery
a General Anesthesia
Use of the Combitube is indicated in routine surgery in patients for whom conventional intubation is not mandatory, such as singers and actors who may be afraid of damage to the vocal cords by endotracheal intubation, or in patients with rheumatoid arthritis with atlantoaxial subluxation. The main advantages of the Combitube in elective and emergency surgery are higher insertion and ventilation rates, reliable protection of the airway against regurgitation and aspiration of gastric contents (e.g., patients with a full stomach, gynecologic laparoscopy), and ventilation and oxygenation against high airway pressures (e.g., obesity, laryngospasm, bronchospasm). As with emergency intubation, it is especially suitable in patients with difficult anatomic conditions. When endotracheal intubation cannot be performed immediately, the Combitube should be considered (Box 27-1). The main advantage in the case of failed intubation or ventilation is immediate esophageal insertion of the Combitube under direct vision without removing the laryngoscope.
Box 27-1 Suggested Indications for Use of the Combitube in Anesthesia and Emergencies
1. The patient’s head does not have to be placed in the traditional sniffing position, as recommended for conventional endotracheal intubation. The patient’s head should remain in a neutral position that allows free movement of the lower jaw. Depending on the situation, the chin may be pushed toward the patient’s chest. Some clinicians prefer to extend the head or to use a small cushion. In patients with a cervical spine injury, the Combitube allows airway management while avoiding mobilization of the neck.
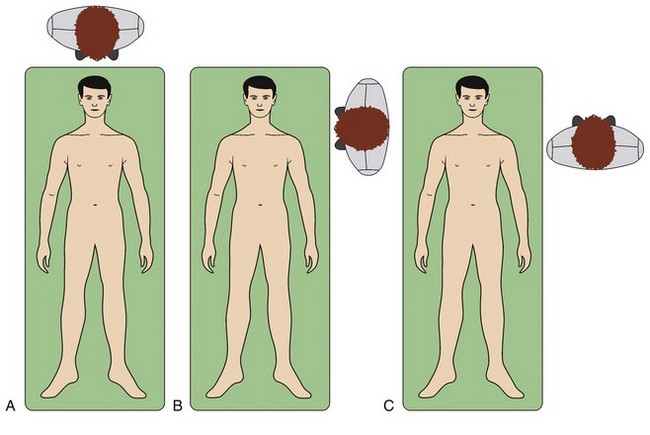
2. The position of the operator (Fig. 27-9) may be behind the patient, especially when a laryngoscope is used (see Fig. 27-9A); to the side of the patient’s head (see Fig. 27-9B); or face to face, when the operator stands beside the patient’s thorax and faces the patient (see Fig. 27-9C). In all three positions, it is necessary to insert the Combitube with a curved downward-caudal movement.
3. During elective surgery, it is always necessary to achieve an adequate depth of anesthesia, with or without additional relaxation. One half of the intubating dose of a neuromuscular blocking agent may be enough to ensure a smooth insertion.18 Gaitini and colleagues have used the Combitube in patients with controlled mechanical ventilation and in spontaneously breathing patients without relaxation.18 However, grasping and elevating the epiglottis with the fingers during insertion may reduce the need for relaxation.
4. Recommended induction agents are propofol or sevoflurane, with or without opioids.37 In a study of 50 female patients undergoing gynecologic laparoscopy, Urtubia and associates successfully inserted the Combitube in 100% of cases using inhalational induction with sevoflurane as the sole agent,38 without opioids or neuromuscular blockade. Use of a laryngoscope is recommended to avoid damage to the oral and pharyngeal mucosa. Nevertheless, with a well-performed blind insertion technique and an adequate level of anesthesia, the risk of damage is comparable to that with the laryngeal mask airway (LMA) or the ETT in terms of postoperative sore throat (16% to 25%).18,24,27 With the laryngoscope, the Combitube is then intentionally introduced into the esophagus. When endotracheal intubation fails, a Combitube can be placed under direct visualization with the laryngoscope still in the patient’s mouth.
5. Another method that may facilitate Combitube insertion and minimize insertion trauma is warming the Combitube in a bottle of warm saline or water, similar to the procedure performed with an ETT for nasal intubation. This technique also allows Combitube insertion without additional application of lubricant.
6. The minimal-volume technique should be applied in elective cases and in emergencies after stabilization of the patient. Studies have shown that adequate sealing of the oropharyngeal balloon can be achieved with 40 to 85 mL of air for the SA Combitube.18,24,27,38–41 Gaitini and colleagues reported that the mean inflation volume of the oropharyngeal balloon at which an air leak was first observed was 45.5 ± 12.3 mL for the 37-F Combitube and 48.1 ± 12.1 mL for the 41-F Combitube.40 The balloon should be initially filled with 40 mL of air only. If a tight seal can be achieved as evaluated by auscultation, comparable to inspiratory and expiratory tidal volumes and the flow-volume curve, the volume is not increased. If a leak is observed, additional increments of 10 mL of air each are added into the balloon until a tight seal is confirmed. The volumes of the oropharyngeal balloon also must be adjusted with the use of nitrous oxide and volatile anesthetics.
b Awake Intubation
In an experiment on himself, Panning showed that the Combitube can be inserted easily with local pharyngeal anesthesia.42 Keller and coworkers inserted the Combitube in four awake volunteers with topical anesthesia.43 Nevertheless, unless an urgent insertion is required, the Combitube should always be inserted when gag reflexes are suppressed because of the risk of mucosal damage or vomiting.
c Replacement of the Combitube
The Combitube may be left in place for up to 8 hours.44 Although emergency and routine surgical procedures may be successfully carried out during this period, the Combitube is not intended for long-term ventilation, because the pressure on the pharyngeal mucosa may be harmful. We recommend replacing the Combitube after a maximum duration of 8 hours. Replacement of the Combitube in the esophageal position by an ETT can be performed in several ways with no danger of aspiration:
1. While the distal cuff remains inflated, deflate the oropharyngeal balloon completely, with the Combitube remaining in the esophagus. Displace the Combitube to the left corner of the mouth, and insert an ETT by laryngoscopy or fiberoptic intubation.45 After successful placement of the ETT, insert a suction catheter through the tracheoesophageal lumen into the esophagus, and during continuous suctioning, deflate the distal cuff, and remove the Combitube. If ETT insertion is impossible, push the Combitube back into its original midline position, reinflate the oropharyngeal balloon, and continue ventilating through the longer no. 1 lumen (blue) of the Combitube until the next endotracheal intubation attempt or until a surgical airway is established.
2. Gaitini and associates described another method.46 The oropharyngeal balloon is partly deflated according to the minimal-volume technique so that the least amount of air allows adequate sealing of the oral and nasal cavities. During continued ventilation through the no. 1 lumen, a fiberoptic bronchoscope mounted with an ETT is introduced through the patient’s mouth. Without a time limit, the bronchoscope may be advanced into the trachea. The unique feature of this method is that ventilation is not interrupted during the entire replacement procedure. All the patients in this study had Mallampati class III or IV oral cavity anatomy.
3. The Combitube may be replaced by surgical means, such as cricothyrotomy or tracheostomy.47 These were the first surgical procedures performed with the Combitube. An advantage of this method is that the trachea is not occupied by an ETT, and ventilation can be continued while the surgical airway is established. A disadvantage is that the trachea is not protected against aspiration of blood generated during the surgical procedure.
4. If there is no danger of aspiration, the Combitube may be removed and replaced by conventional means (e.g., laryngoscopy, bronchoscopy). This approach may be advantageous because intubation around the Combitube can be difficult. In a cadaver study, the laryngeal view with and without the Combitube in place has been compared and the difficulty of intubation around the device evaluated.48 Nine participants in an airway workshop placed 37-F Combitubes in eight non-embalmed cadavers. The pharyngeal balloon was deflated and laryngoscopy attempted with the Combitube in place. Each operator assessed the percentage of glottic opening (POGO) score and tried to pass a tracheal tube around the device. Difficulty of tube passage was rated by the operator. The Combitube was then removed and laryngoscopy (and POGO scoring) repeated without the device. POGO scores with and without the Combitube averaged 61% (95% confidence interval [CI], 49% to 73%) and 92% (CI, 89% to 95%), respectively. Fourteen (19%) of 72 intubation attempts with the Combitube failed. Major difficulty was reported for 22 (31%) of 72 attempts, and minor difficulty for 34 (47%) of 72. The investigators concluded that a previously placed Combitube significantly worsened the laryngeal view at laryngoscopy and prevented intubation in 19% of cases in this cadaver study. They suggest that removal of the Combitube is warranted if any difficulty with laryngoscopy is anticipated or encountered.
5. Harrison and colleagues described the successful replacement of the Combitube with an ETT by retrograde intubation.49 The retrograde intubation was successfully performed without removing an in situ Combitube.
6. A Combitube in the tracheal position can be replaced by an ETT. After lubrication, a pediatric (8-F) tracheal tube exchanger (Cook Critical Care, Bloomington, IN) is introduced into the tracheoesophageal lumen through the shorter no. 2 lumen (transparent) into the trachea, the Combitube is removed, and an ETT is advanced using the tube exchanger as a guide.50,51 If not contraindicated, laryngoscopy should be performed, to facilitate advancement of the ETT through the glottis.
3 Advantages
The Combitube has a wide range of applications and advantages (Box 27-2). Those benefiting from its use include anesthesiologists and physicians in emergency departments,18,19,23 paramedics and emergency medical technicians,19,50,52–57 combat medics,58 parkmedics,59 and physicians in private practice (e.g., responding to anaphylactic reactions).28,31 Cardiac arrests usually do not occur under ideal circumstances, and CPR often is performed in awkward locations, poorly lighted areas, and with limited access to the patient’s head. Because the Combitube can be inserted without a laryngoscope, establishment of a patent airway is not hampered by adverse environmental factors or staff unskilled in endotracheal intubation.27 It is safe against aspiration, and high ventilatory pressures may be applied.
Box 27-2 Advantages of the Combitube and EasyTube
• Noninvasive compared with cricothyrotomy
• Universal size (37-F Small Adult Combitube fits patients 4 to 6.5 ft)18,23,104
• Universal model (one type only)
• Easy to learn, even by untrained personnel58,68,110,129,130
• No preparations necessary; tube and syringes are ready to use
• Helpful under difficult conditions of space and illumination
• Simultaneous fixation after inflation of the oropharyngeal balloon
• Works in the tracheal or esophageal position
• Active decompression of the esophagus and stomach
• Minimized risk of aspiration22,36,38,57,101,106
• Controlled mechanical ventilation possible at high ventilation pressures (≤50 cm H2O)19,24,27,36,51,93,101
• Independent of power supply (e.g., batteries of laryngoscope)
• Well suited for obese patients76,140
• May be used in paralyzed patients who cannot be intubated or mask ventilated
• Only device for insertion in patients with trismus and limited mobility of cervical spine and those with combined pathologic conditions, such as trismus plus limited mobility of the spine and trismus plus tongue edema129
• Fast, safe, and easy to use with successful skill retention129,130
There is no need for additional fixation of the Combitube after inflation of the oropharyngeal balloon, because the anterior upper wall of the oropharyngeal balloon lies just behind the posterior end of the hard palate, thereby guaranteeing strong anchoring during ventilation and transportation. Providing a more secure airway is an attractive advantage of the Combitube compared with other devices used during transportation of emergency patients. Studies have shown that the Combitube is easy to learn and that the skills are retained over time.57
4 Disadvantages
A potential disadvantage of the Combitube is that suctioning tracheal secretions is impossible in the esophageal position. However, studies of use of the esophageal obturator airway in cardiac arrest patients have shown that the outcome of those cases is not statistically different compared with cases in which endotracheal intubation is used.5,6 The Combitube is designed to bridge the short gap between the prehospital setting and admission of the patient to the emergency department. If prolonged ventilation is required, glycopyrronium bromide may be administered to suppress tracheal secretions (e.g., during surgery). Krafft and colleagues have described a redesigned Combitube in which two proximal anterior holes are replaced by one large hole, allowing a bronchoscope to pass for inspection and suctioning of the trachea and as a means for replacing the Combitube using a guidewire.60
6 Complications
Ovassapian and coworkers observed livid discoloration of the tongue during ventilation with the Combitube in a few patients without further sequelae.45 Tongue engorgement was described after 4 hours of Combitube use.61 In an out-of-hospital study with paramedics as rescuers, two lacerations of the esophagus were found in autopsies of cardiac arrest patients ventilated with the Combitube.62 However, the investigators found that the distal cuff was overfilled with 20 to 40 mL of air (instead of 10 ± 1 mL). As outlined in the instructions, the Combitube should not be advanced with use of force. Klein and associates reported an esophageal rupture after insertion of a Combitube, stiff suctioning catheter, LMA, laryngoscope, and ETT.35 A traumatic procedure with one or more of these devices probably caused the complication.
Overinflation of the esophageal balloon was described in a case reporting airway obstruction secondary to tracheal compression. In this case, the esophageal balloon was inflated with 22.4 mL according to the computed tomography (CT) measurement.63 Richards reported a case of piriform sinus perforation during the insertion of the Combitube.64 This patient presented with cardiorespiratory arrest due to angioedema, probably caused by treatment with angiotensin-converting enzyme inhibitors. Another case of piriform sinus perforation during Combitube placement was reported by Moser.65
Oczenski and coworkers reported a very high number of complications for cases of elective surgery.66 The total complication rate found by Oczenski’s group66 was fourfold that found in the studies led by Gaitini,18 Hartmann,27 and Urtubia.24 This unexpectedly high rate of complications probably was caused by traumatic maneuvers during airway management, which is in accordance with an 8% rate of pharyngeal hematoma associated with the LMA. Vezina and colleagues retrospectively reviewed medical records of patients with cardiac or respiratory arrest.67 The study was performed in the Quebec City Health Region, where paramedics use the Combitube as a primary airway device for patients with cardiorespiratory arrest. A high incidence of complications was reported.
The study of Oczenski and coworkers demonstrates that all precautions should be considered when there are obvious handling problems.66 When facing difficulties during insertion, a laryngoscope should be used immediately to insert the Combitube intentionally into the esophagus under direct vision.
G Medical Literature
1 Combitube in Cardiac Arrest Patients
a IN-Hospital Studies
Application of the Combitube during CPR has been investigated.14–1621 The first study consisted of two parts.15 The first part considered the blood gas analyses of 19 patients after 15 minutes of ventilation with the Combitube. In the second part, the blood gas analyses of samples taken from 12 patients during ventilation with the Combitube were compared with those taken during subsequent ventilation with a conventional ETT. Blood gas analyses showed higher arterial oxygen pressures with the Combitube than with an ETT (124 ± 33 versus 103 ± 30 mm Hg; P = 0.001). Carbon dioxide pressure was not significantly different.
A second study reported the use of the Combitube during in-hospital CPR.14 In a randomized sequence, the Combitube or a conventional ETT was used in 43 patients. After stabilization of the patients, each tube was replaced with the other type of tube. Blood gas analyses revealed increased oxygen tensions during Combitube ventilation, and the intubation time was significantly shorter with the Combitube.
Another study evaluated the safety and effectiveness of the 41-F Combitube as used by ICU nurses under medical supervision compared with an ETT established by ICU physicians during CPR.68 The intubation time was shorter for the Combitube, and results of blood gas determinations for each device were comparable, although arterial oxygen tension was slightly higher during ventilation with the Combitube. The study suggests that the Combitube as used by ICU nurses is as effective as the ETT as used by ICU physicians during CPR.
Related posts:
 Prehospital Airway Management
Prehospital Airway Management
 Medical-Legal Considerations: The ASA Closed Claims Project
Medical-Legal Considerations: The ASA Closed Claims Project
 Performance of Rigid Bronchoscopy
Performance of Rigid Bronchoscopy
 Nonintubation Management of the Airway: Airway Maneuvers and Mask Ventilation
Nonintubation Management of the Airway: Airway Maneuvers and Mask Ventilation

Full access? Get Clinical Tree


