Type
Causes
Clinical findings
Anatomic
External compression from an aberrant right subclavian artery
Pyriform sinus
Singing, yelling, trumpet playing, recent endoscopy
Marked mediastinal and cervical subcutaneous emphysema
Anastomotic
Leakage at or near the site of a surgical anastomosis
History of surgically created esophageal anastomosis
Boerhaave’s
Vomiting, straining, retching, weight lifting, hyperemesis, seizures causing a full-thickness tear at the gastroesophageal junction
Characteristic longitudinal tear on the left side of the esophagus, typically in the distal 1/3 segment
Mucosal defect typically longer than muscular defect
Iatrogenic
Endoscopic: Ablation, dilation, sclerotherapy, instrumentation
Surgical: Esophageal surgery, foregut cyst decortication, spine surgery
Recent history of surgery or endoscopy
Traumatic
Penetrating or blunt trauma to neck or torso
Strong association with neck hyperextension
Cancer
Perforation of an esophageal tumor
Erosion of surrounding tumor through esophageal wall
Gas near or abutting the tumor on imaging
Paraesophageal hernia
Incarceration with necrosis of the distal esophagus
Evidence of left pleural effusion or abdominal fluid on imaging studies
Foreign body
Ingestion of a substance (i.e., chicken bone) that becomes lodged
Impaction at a stricture
Esophageal webs
Eosinophilic esophagitis
Upper esophageal impaction at the sphincter
Esophagitis
Inflammation and erosion of ulceration
Zollinger–Ellison syndrome
Barrett’s ulcer
Infection (Candida, Herpes simplex, viruses, CMV)
Immunocompromised patient
Ingestion
Ingestion of caustic substance
Drug ingestion/impaction
Tetracycline
Potassium
Quinidine
NSAIDS
Sustained-release formulations
Spontaneous esophageal perforation, commonly known as Boerhaave’s syndrome, results from abrupt increases in intraesophageal pressure. It was originally described by Herman Boerhaave in 1724, in a pamphlet detailing his postmortem observations of Baron de Wassenaer, the Grand Admiral of Holland. Though Boerhaave’s syndrome has historically come to be linked with violent emesis following unrestrained imbibition or food consumption, the Baron suffered a fatal esophageal rupture as a result of self-induced vomiting in an attempt to relieve the discomfort of indigestion [4]. Spontaneous perforations associated with weight lifting, childbirth, seizures, and defecation have been reported, and likely bear a similar physiologic origin.
The superficial course of both the cervical and thoracic esophagus renders them susceptible to injury from penetrating trauma. Additionally, gunshot wounds can also inflict indirect thermal injury easily missed at initial examination that can subsequently become the site of a rupture. Esophageal disruption can likewise occur in the setting of blunt traumatic injuries. Putative mechanisms include torsive and stretching forces, as well as rapid acceleration with injury occurring at fixed points. Ingestion of caustic materials, broadly classified as acidic or alkaline, can also result in esophageal perforation. This is most common with alkaline consumption, as these agents are both more palatable and cause a liquefactive necrosis with a propensity for transmural progression of the injury. Although acid ingestion results in a coagulative necrosis with less potential for penetration, perforation can occur.
Acute inflammation and infection can also lead to perforation of a weakened esophageal wall, particularly in the immunocompromised patient. One noteworthy etiology is eosinophilic esophagitis, characterized by unexplained focal penetration of eosinophils. Multiple reports of spontaneous perforation in this setting exist [5, 6].
Presentation
The clinical signs and symptoms of esophageal perforation are largely dependent upon the anatomic location of the defect. Fever, tachycardia, tachypnea, dyspnea, shock, and leukocytosis are frequently present regardless of the site of the injury. Crepitus, indicative of underlying subcutaneous emphysema, suggests a perforation in the neck or pyriform sinus. Additionally, these patients may describe neck pain of varying severity, vocal disturbances classically described as a prominent “nasal” tonality, dysphagia, or bleeding through the mouth. Perforations of the thoracic or abdominal esophagus often result in vomiting, chest and/or back pain, dyspnea, dysphagia, and bleeding. In addition, defects of the intra-abdominal esophagus commonly cause abdominal pain and distention. “Mackler’s Triad” denotes the classic presenting syndrome of patients with spontaneous esophageal rupture, and includes vomiting, lower chest pain, and subcutaneous emphysema. The Anderson Triad, likewise suggestive of spontaneous esophageal rupture, includes subcutaneous emphysema, rapid respirations, and abdominal rigidity.
Evaluation
Evaluation of the patient with suspected esophageal perforation begins with a detailed history and physical examination. Particular attention should be given to any recent history of instrumentation or trauma to the neck or torso, quantitative and qualitative assessment of recent food and liquid consumption, evidence of malignancy such as recent weight loss or dysphagia, or any signs of progressing sepsis. Hemodynamic instability should be immediately addressed with placement of large-bore intravenous catheters and fluid administration. Once esophageal perforation is suspected, antero-posterior and lateral upright chest and abdominal radiographs should be obtained without delay. Radiographic findings suspicious for perforation include subcutaneous emphysema, the presence of pleural effusions, pneumomediastinum, hydro/pneumothorax, and pleural thickening. Radiographs are particularly useful in the setting of suspected iatrogenic perforation, as they may prove diagnostic in up to 80% of these patients. Furthermore, radiographs have utility in terms of localization of the defect; a right pleural effusion suggests a mid-esophageal perforation, while a left effusion portends a lower esophageal lesion.
The gold standard for diagnosis of perforation is a contrast swallow study, done in the presence of the treating surgeon. Performed fluoroscopically, the patient should be oriented obliquely relative to the source and remain in a standing, semierect position, which will facilitate the detection of small leaks (Fig. 14.1 through Fig. 14.5). Given the risk of severe pneumonitis associated with gastrograffin aspiration, angiography agents are preferred. Barium use can complicate future imaging in the patient due to persistence of the substance in the esophagus for several days, and should only be used if an obvious perforation is not detected on initial swallow evaluation with a water-soluble contrast agent. Although essential in the initial evaluation of suspected esophageal perforation, the false negative rate of contrast radiography approaches thirty percent.
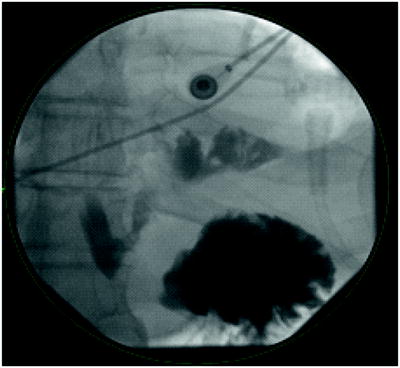
Fig. 14.1



Contrast esophagram of a Boerhaave perforation of the esophagus at the gastroesophageal junction resulting in left pleural contamination
Related posts:





Full access? Get Clinical Tree
