ergotamine and dihydroergotamine (6,112,114). For ergotamine, the hypertensive response is caused by increased total peripheral resistance (116). Basal cerebral blood flow (CBF) and acetazolamide-stimulated CBF also is unchanged after both ergotamine and dihydroergotamine (6). Basal myocardial blood flow also is unchanged after intravenous ergotamine, but the coronary vasodilator reserve decreases, probably by an effect on the microcirculation (38). In contrast to the short-lasting (about 3 hours) effect on blood pressure, ergotamine causes a long-lasting (at least 24 hours) vasoconstriction of leg arteries (112,114,122). A similar long-lasting venoconstrictor effect (at least 8 hours) has been observed after a single dose of dihydroergotamine (5). For dihydroergotamine no effect on peripheral arteries was found (6). An important feature of ergotamine and dihydroergotamine, observed in vitro is that their effect on blood vessels is resistant to repeated wash (79,84,87), which appears to be caused mainly by slow diffusion from the receptor biophase; therefore,
their effects last far longer than can be expected from plasma concentrations (5,118).
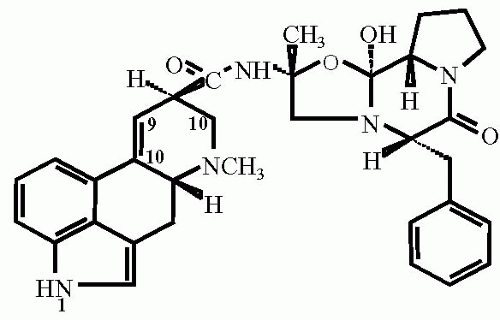 FIGURE 50-1. |
TABLE 50-1 Receptor Profile of Ergotamine and Dihydroergotamine as Compared to Sumatriptan | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Related posts:







Full access? Get Clinical Tree


