CHAPTER 27
Epistaxis
(Nosebleed)
Presentation
The patient generally arrives in the ED or urgent care center with active bleeding from his nose, or he may be spitting up blood that is draining into his throat. There may be a report of minor trauma, such as sneezing, nose blowing, or nose picking. On occasion, the hemorrhage has stopped, but the patient is concerned because the bleeding has been recurrent. In rare instances, the bleeding may be brisk requiring resuscitation. Bleeding is most commonly present on the anterior aspect of the nasal septum, within the Kiesselbach area or on the inferior turbinate. Sometimes, especially with posterior epistaxis, a specific bleeding site cannot be determined.
What To Do:
 If significant blood loss is suspected, there are abnormal vital signs, or there is continued brisk bleeding, gain vascular access and administer crystalloid IV solution. Provide continuous cardiac monitoring and pulse oximetry. Ensure an adequate airway and oxygenation. Controlling significant hemorrhage should always take precedence over obtaining a detailed history or visualization of the specific bleeding site.
If significant blood loss is suspected, there are abnormal vital signs, or there is continued brisk bleeding, gain vascular access and administer crystalloid IV solution. Provide continuous cardiac monitoring and pulse oximetry. Ensure an adequate airway and oxygenation. Controlling significant hemorrhage should always take precedence over obtaining a detailed history or visualization of the specific bleeding site.
 With all nosebleeds, have the patient maintain compression on the nostrils by pinching with a gauze sponge, while all equipment and supplies are being assembled at the bedside. If the patient is unable to pinch the nostrils, a compression device can be made by taping two tongue blades together at one end and placing the other end across the soft portion of the nose. Commercially available nasal clips may also be used.
With all nosebleeds, have the patient maintain compression on the nostrils by pinching with a gauze sponge, while all equipment and supplies are being assembled at the bedside. If the patient is unable to pinch the nostrils, a compression device can be made by taping two tongue blades together at one end and placing the other end across the soft portion of the nose. Commercially available nasal clips may also be used.
 Use of a headlight with a focused beam will allow you to have both hands free for examination and manipulation while ensuring good lighting and visualization.
Use of a headlight with a focused beam will allow you to have both hands free for examination and manipulation while ensuring good lighting and visualization.
 Have the patient sit upright (unless hypotensive). If necessary, sedate the patient with a mild tranquilizer, such as lorazepam (Ativan) or midazolam (Versed). Cover the patient and yourself to protect clothing. Follow universal precautions by using gloves and wearing protective eyewear and a surgical mask.
Have the patient sit upright (unless hypotensive). If necessary, sedate the patient with a mild tranquilizer, such as lorazepam (Ativan) or midazolam (Versed). Cover the patient and yourself to protect clothing. Follow universal precautions by using gloves and wearing protective eyewear and a surgical mask.
 Prepare 5 mL of a solution to anesthetize and vasoconstrict the nasal mucosa. This can consist of 4% cocaine alone or a 1:1 mixture of 2% tetracaine and a vasoconstrictor such as 1% phenylephrine or 0.05% oxymetazoline.
Prepare 5 mL of a solution to anesthetize and vasoconstrict the nasal mucosa. This can consist of 4% cocaine alone or a 1:1 mixture of 2% tetracaine and a vasoconstrictor such as 1% phenylephrine or 0.05% oxymetazoline.
 Form two elongated cotton pledgets (using ¼ of a cotton ball for each pledget), and soak them in the prepared solution.
Form two elongated cotton pledgets (using ¼ of a cotton ball for each pledget), and soak them in the prepared solution.

 Instruct the patient to blow the clots from his nose, and then quickly inspect for a bleeding site using the nasal speculum and Frazier suction tip. Be sure to orient the nasal speculum vertically to avoid pain. Clear out any clots or foreign bodies (Figure 27-1). The bleeding may be too brisk to indentify a bleeding site at this time, and therefore inspection may be delayed until vasoconstriction has slowed the hemorrhage.
Instruct the patient to blow the clots from his nose, and then quickly inspect for a bleeding site using the nasal speculum and Frazier suction tip. Be sure to orient the nasal speculum vertically to avoid pain. Clear out any clots or foreign bodies (Figure 27-1). The bleeding may be too brisk to indentify a bleeding site at this time, and therefore inspection may be delayed until vasoconstriction has slowed the hemorrhage.

Figure 27-1 The patient must blow the clots from his nose prior to the insertion of medicated cotton pledgets.
 Insert the medicated cotton pledgets as far back as possible into both nostrils (or one nostril, if the bleeding site is evident) using the bayonet forceps (Figure 27-2).
Insert the medicated cotton pledgets as far back as possible into both nostrils (or one nostril, if the bleeding site is evident) using the bayonet forceps (Figure 27-2).
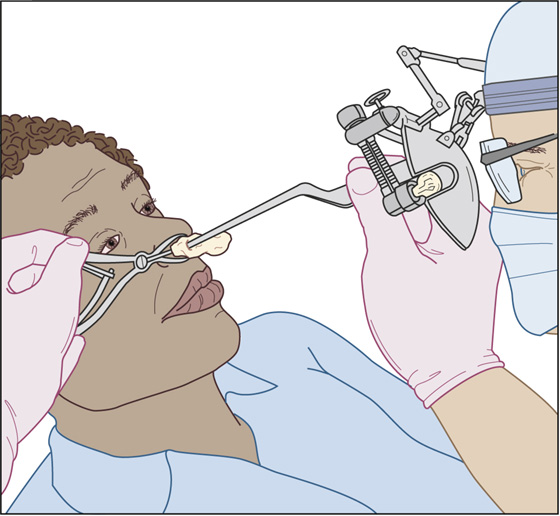
Figure 27-2 Insertion of medicated cotton pledgets.
 Allow the patient to relax with the pledgets in place for approximately 5 to 20 minutes, applying nose clips or having the patient pinch the anterior half of his or her nose.
Allow the patient to relax with the pledgets in place for approximately 5 to 20 minutes, applying nose clips or having the patient pinch the anterior half of his or her nose.
 During this lull, inquire about the patient’s history of nosebleeds or other medical problems, the pattern of this nosebleed, which side the bleeding seems to be coming from, use of any blood thinning medications or intranasal products (legal or illegal). Often, no cause for the bleeding can be identified, but when there is diffuse oozing, multiple bleeding sites, or recurrent bleeding, or if the patient is taking an anticoagulant, a hematologic evaluation should be performed (complete blood count [CBC] and international normalized ratio [INR]). Type and cross match the patient if significant blood loss is suspected.
During this lull, inquire about the patient’s history of nosebleeds or other medical problems, the pattern of this nosebleed, which side the bleeding seems to be coming from, use of any blood thinning medications or intranasal products (legal or illegal). Often, no cause for the bleeding can be identified, but when there is diffuse oozing, multiple bleeding sites, or recurrent bleeding, or if the patient is taking an anticoagulant, a hematologic evaluation should be performed (complete blood count [CBC] and international normalized ratio [INR]). Type and cross match the patient if significant blood loss is suspected.
 In most cases, active bleeding will stop with the use of the vasoconstrictor alone. The cotton pledgets can be removed and the nasal cavity inspected using the nasal speculum and head lamp. Gently inserting the nasal speculum and spreading the naris vertically will permit visualization of most anterior bleeding sources. If bleeding continues, insert another pair of medicated cotton pledgets, and repeat this procedure with more prolonged nasal compression. (Again, commercially available nasal clips can accomplish this for your patient.)
In most cases, active bleeding will stop with the use of the vasoconstrictor alone. The cotton pledgets can be removed and the nasal cavity inspected using the nasal speculum and head lamp. Gently inserting the nasal speculum and spreading the naris vertically will permit visualization of most anterior bleeding sources. If bleeding continues, insert another pair of medicated cotton pledgets, and repeat this procedure with more prolonged nasal compression. (Again, commercially available nasal clips can accomplish this for your patient.)
 Although infrequent, there are times when the patient is hemorrhaging so briskly that the nose must be tamponaded using a balloon catheter or other intervention without inspection, topical anesthesia, or attempted cautery.
Although infrequent, there are times when the patient is hemorrhaging so briskly that the nose must be tamponaded using a balloon catheter or other intervention without inspection, topical anesthesia, or attempted cautery.
 If the bleeding point can be located and the bleeding is not too brisk, attempt to cauterize a 0.5-cm area of mucosa around the bleeding site with a silver nitrate stick, and then cauterize the site itself. If there is an individual vessel bleeding rapidly, hold the tip of the cautery stick on top of that vessel with pressure for up to 20 seconds or until the bleeding stops (Figure 27-3).
If the bleeding point can be located and the bleeding is not too brisk, attempt to cauterize a 0.5-cm area of mucosa around the bleeding site with a silver nitrate stick, and then cauterize the site itself. If there is an individual vessel bleeding rapidly, hold the tip of the cautery stick on top of that vessel with pressure for up to 20 seconds or until the bleeding stops (Figure 27-3).
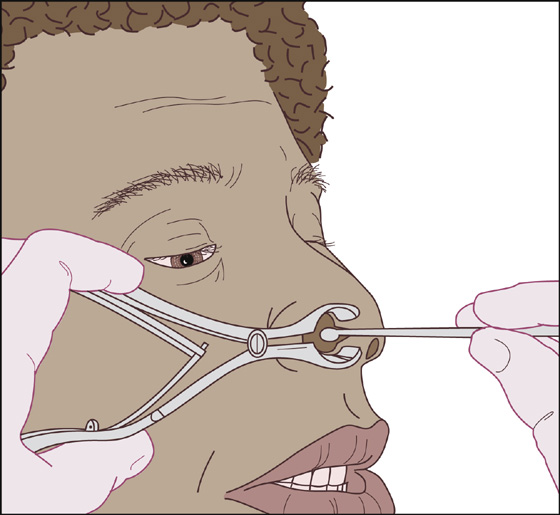
Figure 27-3 Cauterize mucosa with a silver nitrate stick.
 If the bleeding stops with cauterization, observe the patient for 15 to 30 minutes. The cauterized area can then be covered with absorbable gelatin foam (Gelfoam), oxidized cellulose (Surgicel), or antibiotic ointment.
If the bleeding stops with cauterization, observe the patient for 15 to 30 minutes. The cauterized area can then be covered with absorbable gelatin foam (Gelfoam), oxidized cellulose (Surgicel), or antibiotic ointment.
 If the bleeding point cannot be located or if bleeding continues after cauterization, nonabsorbable or absorbable packing may be used.
If the bleeding point cannot be located or if bleeding continues after cauterization, nonabsorbable or absorbable packing may be used.
 The two most common nonabsorbable packings are the sponge and the balloon. The sponge is made of hydroxylated polyvinyl acetate, is compressed, and expands into a soft sponge when wet (Merocel sponge, Medtronic, Minneapolis, Minn.). The balloon consists of an inflatable tube covered with a mesh of hemostatic carboxymethyl cellulose hydrocolloid (Rapid Rhino, Arthro Care, Austin, Tex.).
The two most common nonabsorbable packings are the sponge and the balloon. The sponge is made of hydroxylated polyvinyl acetate, is compressed, and expands into a soft sponge when wet (Merocel sponge, Medtronic, Minneapolis, Minn.). The balloon consists of an inflatable tube covered with a mesh of hemostatic carboxymethyl cellulose hydrocolloid (Rapid Rhino, Arthro Care, Austin, Tex.).
 There are short and long varieties of the sponge and balloon, as well as balloons with anterior and posterior compartments. Longer packs can be used for patients suspected of posterior bleeding.
There are short and long varieties of the sponge and balloon, as well as balloons with anterior and posterior compartments. Longer packs can be used for patients suspected of posterior bleeding.
 To use the sponge, coat it lightly with antibiotic ointment to provide some lubrication, and insert along the floor of the nasal cavity into the already anesthetized nose. If you are having trouble fitting the sponge, it can be trimmed.
To use the sponge, coat it lightly with antibiotic ointment to provide some lubrication, and insert along the floor of the nasal cavity into the already anesthetized nose. If you are having trouble fitting the sponge, it can be trimmed.
 Leave a bit of the sponge exposed to allow easy removal (some sponges have a string attached, which can be taped to the face). Expand the sponge, after full insertion, with a small amount of saline. (You can also use the vasoconstricting solution for added hemostasis.)
Leave a bit of the sponge exposed to allow easy removal (some sponges have a string attached, which can be taped to the face). Expand the sponge, after full insertion, with a small amount of saline. (You can also use the vasoconstricting solution for added hemostasis.)
 The balloon pack is less comfortable for the patient after insertion but can exert more local pressure to the bleeding site. Possibly the most comfortable of these commercially available nasal tampons and the easiest to insert is the gel-coated, balloon-inflated Rapid Rhino nasal pack (ArthroCare, Austin, Tex.).
The balloon pack is less comfortable for the patient after insertion but can exert more local pressure to the bleeding site. Possibly the most comfortable of these commercially available nasal tampons and the easiest to insert is the gel-coated, balloon-inflated Rapid Rhino nasal pack (ArthroCare, Austin, Tex.).
 To insert the nasal balloon, choose the appropriate length and soak the balloon in water for 30 seconds to gel the colloid. Insert the entire length of the balloon along the floor of the anesthetized nasal cavity. If you do not insert the entire balloon into the nose, it will work its way out of the nose during inflation. Inflate the balloon with air until the cuff feels firm or the patient experiences mild discomfort. The air in the balloon may later be adjusted for patient comfort and control of bleeding. Tape the free end of the pilot cuff to the patient’s cheek.
To insert the nasal balloon, choose the appropriate length and soak the balloon in water for 30 seconds to gel the colloid. Insert the entire length of the balloon along the floor of the anesthetized nasal cavity. If you do not insert the entire balloon into the nose, it will work its way out of the nose during inflation. Inflate the balloon with air until the cuff feels firm or the patient experiences mild discomfort. The air in the balloon may later be adjusted for patient comfort and control of bleeding. Tape the free end of the pilot cuff to the patient’s cheek.
 An alternative anterior pack, though difficult and time consuming to place, can be made from up to 6 feet of ½-inch Vaseline gauze. Cover the gauze with antibiotic ointment and insert it with a bayonet forceps. Start with three or four layers in accordion fashion on the floor of the anesthetized nasal cavity, placing the gauze as far posterior as possible, pressing it down with each layer. This method should be reserved for situations in which the sponge, balloon and absorbable packing have failed or are not available (Figure 27-4).
An alternative anterior pack, though difficult and time consuming to place, can be made from up to 6 feet of ½-inch Vaseline gauze. Cover the gauze with antibiotic ointment and insert it with a bayonet forceps. Start with three or four layers in accordion fashion on the floor of the anesthetized nasal cavity, placing the gauze as far posterior as possible, pressing it down with each layer. This method should be reserved for situations in which the sponge, balloon and absorbable packing have failed or are not available (Figure 27-4).
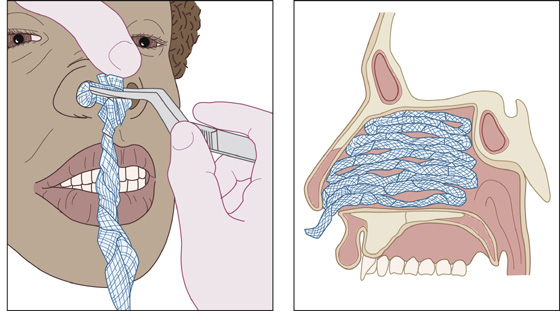
Figure 27-4 Packing the nasal cavity with ribbon gauze.
 An alternative to using nonabsorbable packing is to use absorbable packing material. The advantages are that there is nothing to remove later, and there is more patient comfort. The disadvantages are a higher initial cost and lack of tamponading effect.
An alternative to using nonabsorbable packing is to use absorbable packing material. The advantages are that there is nothing to remove later, and there is more patient comfort. The disadvantages are a higher initial cost and lack of tamponading effect.
 Choices of absorbable packing material include oxidized cellulose (Surgicel, Johnson & Johnson, New Brunswick, N.J.), purified bovine collagen (Gelfoam, Pfizer, New York, N.Y.), both of which come in sheets and can be pressed against the bleeding site. Porcine gelatin (Surgiflo, Johnson & Johnson, New Brunswick, N.J.) and bovine gelatin-human thrombin (Floseal, Baxter, Deerfield, Ill.) are materials that can be mixed into a paste and applied to the nasal mucosa.
Choices of absorbable packing material include oxidized cellulose (Surgicel, Johnson & Johnson, New Brunswick, N.J.), purified bovine collagen (Gelfoam, Pfizer, New York, N.Y.), both of which come in sheets and can be pressed against the bleeding site. Porcine gelatin (Surgiflo, Johnson & Johnson, New Brunswick, N.J.) and bovine gelatin-human thrombin (Floseal, Baxter, Deerfield, Ill.) are materials that can be mixed into a paste and applied to the nasal mucosa.
 If the hemorrhage does not stop after placing adequate packing anteriorly, unilateral or bilateral posterior packing or nasal balloons should be inserted. A lubricated double-balloon device (Epistat [Medtronic Xomed, Jacksonville, Fla.], Nasostat [Sparta, Pleasanton, Calif.]) (Figure 27-5) is passed into the affected nostril in that same way as the anterior balloon. The posterior balloon is inflated first with the manufacturer’s recommended volume of normal saline, and the anterior portion of the device is withdrawn so that the posterior balloon seats snugly in the posterior nasal cavity to tamponade any bleeding. The anterior balloon is then inflated with the recommended volume of saline to prevent the posterior balloon from becoming unseated and possibly obstructing the airway.
If the hemorrhage does not stop after placing adequate packing anteriorly, unilateral or bilateral posterior packing or nasal balloons should be inserted. A lubricated double-balloon device (Epistat [Medtronic Xomed, Jacksonville, Fla.], Nasostat [Sparta, Pleasanton, Calif.]) (Figure 27-5) is passed into the affected nostril in that same way as the anterior balloon. The posterior balloon is inflated first with the manufacturer’s recommended volume of normal saline, and the anterior portion of the device is withdrawn so that the posterior balloon seats snugly in the posterior nasal cavity to tamponade any bleeding. The anterior balloon is then inflated with the recommended volume of saline to prevent the posterior balloon from becoming unseated and possibly obstructing the airway.
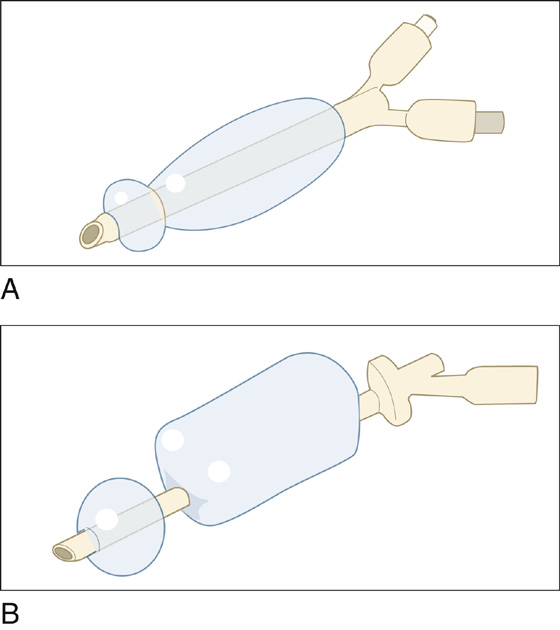
Figure 27-5 Double-balloon devices. A, Epistat. B, Nasostat.
 If a commercial posterior balloon device is not available, a 12-Fr Foley catheter may be used. Insert the catheter into the affected nasal cavity until the balloon is well into the posterior nasal cavity. Inflate the balloon with 5 to 7 mL of saline. Pull the partially inflated balloon anteriorly until it is snug against the posterior turbinates. Finish inflating the balloon with another 5 to 7 mL saline. If there is pain or displacement of the soft palate, remove some of the saline from the balloon. Secure the Foley anteriorly by placing an umbilical clamp over the catheter as it exits the nose. Make sure to pad the nose tissue with gauze to prevent pressure necrosis. An anterior Vaseline gauze pack may then be inserted.
If a commercial posterior balloon device is not available, a 12-Fr Foley catheter may be used. Insert the catheter into the affected nasal cavity until the balloon is well into the posterior nasal cavity. Inflate the balloon with 5 to 7 mL of saline. Pull the partially inflated balloon anteriorly until it is snug against the posterior turbinates. Finish inflating the balloon with another 5 to 7 mL saline. If there is pain or displacement of the soft palate, remove some of the saline from the balloon. Secure the Foley anteriorly by placing an umbilical clamp over the catheter as it exits the nose. Make sure to pad the nose tissue with gauze to prevent pressure necrosis. An anterior Vaseline gauze pack may then be inserted.
 If the bleeding cannot be controlled with all of the above measures, YOU NEED HELP! Contact an ear-nose-throat (ENT) specialist or transfer the patient to a hospital with ENT care. The specialist may use electrocautery, transpalatal injection of vasoconstrictors, endoscopic cautery, surgical ligation, or embolization procedures. While the patient is awaiting specialist care, you must ensure hemodynamic stability using IV fluids or blood, if needed.
If the bleeding cannot be controlled with all of the above measures, YOU NEED HELP! Contact an ear-nose-throat (ENT) specialist or transfer the patient to a hospital with ENT care. The specialist may use electrocautery, transpalatal injection of vasoconstrictors, endoscopic cautery, surgical ligation, or embolization procedures. While the patient is awaiting specialist care, you must ensure hemodynamic stability using IV fluids or blood, if needed.
 If on the other hand, as will most commonly occur, the bleeding has stopped with your interventions, observe the patient for 15 to 30 minutes. If there is no further bleeding from the nares or from the posterior pharynx, the patient may be discharged. If the hemorrhage is suspected to have been large, determine that the patient is not symptomatically orthostatic, and check hemoglobin and hematocrit before discharging.
If on the other hand, as will most commonly occur, the bleeding has stopped with your interventions, observe the patient for 15 to 30 minutes. If there is no further bleeding from the nares or from the posterior pharynx, the patient may be discharged. If the hemorrhage is suspected to have been large, determine that the patient is not symptomatically orthostatic, and check hemoglobin and hematocrit before discharging.
 If a nonabsorbable pack was inserted, the patient should be sent home on a regimen of antibiotics for 4 to 5 days to help prevent a secondary sinusitis and reduce the risk of toxic shock syndrome. Choices of antibiotics include cephalexin (Keflex), amoxicillin/clavulanate (Augmentin), clindamycin (Cleocin), and trimethoprim/sulfamethoxazole (Bactrim).
If a nonabsorbable pack was inserted, the patient should be sent home on a regimen of antibiotics for 4 to 5 days to help prevent a secondary sinusitis and reduce the risk of toxic shock syndrome. Choices of antibiotics include cephalexin (Keflex), amoxicillin/clavulanate (Augmentin), clindamycin (Cleocin), and trimethoprim/sulfamethoxazole (Bactrim).
 The nonabsorbable packs should be removed in 2 to 5 days. Packs for minor bleeds may be removed early; bleeds that are difficult to control or in patients on anticoagulants should be kept in the full 5 days.
The nonabsorbable packs should be removed in 2 to 5 days. Packs for minor bleeds may be removed early; bleeds that are difficult to control or in patients on anticoagulants should be kept in the full 5 days.
 Warn the patient about not sneezing with his mouth closed, bending over, straining, or picking his nose. Provide printed instructions regarding home care.
Warn the patient about not sneezing with his mouth closed, bending over, straining, or picking his nose. Provide printed instructions regarding home care.
 Patients with simple nosebleeds can be referred to their primary care doctor for removal of the packing or for a recheck. If this is a recurrent bleeding episode, or there is concern for a nasal abnormality causing the bleeding, the patient should be referred to an ENT specialist.
Patients with simple nosebleeds can be referred to their primary care doctor for removal of the packing or for a recheck. If this is a recurrent bleeding episode, or there is concern for a nasal abnormality causing the bleeding, the patient should be referred to an ENT specialist.
 If pain is a problem, Tylenol should be suggested and aspirin and other nonsteroidals avoided. Prescribe hydrocodone bitartrate/acetaminophen (Vicodin) if you think the pain will not be controlled with Tylenol.
If pain is a problem, Tylenol should be suggested and aspirin and other nonsteroidals avoided. Prescribe hydrocodone bitartrate/acetaminophen (Vicodin) if you think the pain will not be controlled with Tylenol.
 If the patient returns with mild oozing of blood from around an anterior pack, you may be able to stop the bleeding without removing the pack. Try injecting a vasoconstrictor directly into the sponge (not into the patient), or adding air to a nasal balloon pack.
If the patient returns with mild oozing of blood from around an anterior pack, you may be able to stop the bleeding without removing the pack. Try injecting a vasoconstrictor directly into the sponge (not into the patient), or adding air to a nasal balloon pack.
 When removing a compressed cellulose sponge pack, soften it with 1 to 2 mL of water or saline and wait 5 minutes, thereby reducing trauma, pain, and the incidence of rebleeding.
When removing a compressed cellulose sponge pack, soften it with 1 to 2 mL of water or saline and wait 5 minutes, thereby reducing trauma, pain, and the incidence of rebleeding.
What Not To Do:
Because of the nasopulmonary reflex, arterial oxygen pressure will drop about 15 mm Hg after the nose is packed. Do not send home elderly patients or those with cardiac problems or chronic obstructive pulmonary disease (COPD) without first checking their oxygen saturation. With packing in place, these patients are at risk for desaturation and may need admission.
 Do not waste time trying to locate a bleeding site if brisk bleeding is obscuring your vision in spite of vigorous suctioning. Have the patient blow out any clots and insert the medicated cotton pledgets immediately or go directly to anterior packing.
Do not waste time trying to locate a bleeding site if brisk bleeding is obscuring your vision in spite of vigorous suctioning. Have the patient blow out any clots and insert the medicated cotton pledgets immediately or go directly to anterior packing.
 Do not order routine clotting studies unless there is persistent or recurrent bleeding, use of anticoagulants or other evidence of an underlying bleeding disorder.
Do not order routine clotting studies unless there is persistent or recurrent bleeding, use of anticoagulants or other evidence of an underlying bleeding disorder.
 Do not cauterize or place a painful device in the nose before providing adequate topical anesthesia unless rapid hemorrhaging requires it.
Do not cauterize or place a painful device in the nose before providing adequate topical anesthesia unless rapid hemorrhaging requires it.
 Do not use an inadequate amount of gauze packing, if this method is chosen. It will only serve as a plug in the anterior nares rather than as a hemostatic pack.
Do not use an inadequate amount of gauze packing, if this method is chosen. It will only serve as a plug in the anterior nares rather than as a hemostatic pack.
 Do not discharge a patient as soon as the bleeding stops, but keep him for 15 to 30 minutes more. Look behind the uvula. If there is active blood flow, the bleeding has not been controlled adequately. Posterior epistaxis typically stops and starts cyclically and may not be recognized until all of the aforementioned treatments have failed.
Do not discharge a patient as soon as the bleeding stops, but keep him for 15 to 30 minutes more. Look behind the uvula. If there is active blood flow, the bleeding has not been controlled adequately. Posterior epistaxis typically stops and starts cyclically and may not be recognized until all of the aforementioned treatments have failed.
Epistaxis (Greek for nosebleed) affects people in all age groups but is most common and more troublesome in the elderly. Children tend to bleed secondary to nose picking; adolescents bleed secondary to facial trauma associated with athletic activity or fighting. Epistaxis in the middle-age patient is more often the harbinger of neoplastic disease. Nosebleeds in the elderly are generally the result of underlying vascular fragility in combination with blood-thinning medications.
Nosebleeds are more common in winter, no doubt reflecting the low, ambient humidity indoors and outdoors and the increased incidence of upper respiratory tract infections. In most cases, anterior bleeding is clinically obvious. In contrast, posterior bleeding may be asymptomatic or may present insidiously as nausea, hematemesis, anemia, hemoptysis, or melena.
Causes of epistaxis are numerous; dry nasal mucosa, nose picking, and vascular fragility are the most common causes, but others include trauma, foreign bodies, blood dyscrasias, nasal or sinus neoplasm or infection, septal deformity or perforation, atrophic rhinitis, hereditary hemorrhagic telangiectasis, and angiofibroma. Epistaxis that results from minor blunt trauma in healthy individuals rarely requires any intervention and will spontaneously subside with head elevation alone and avoidance of any nasal manipulation. (Always inspect for a possible septal hematoma.)
High blood pressure may make epistaxis more difficult to control; however, although it is often present with epistaxis, it is rarely the sole precipitating cause. Specific antihypertensive therapy is rarely required and should be avoided in the setting of significant hemorrhage.
Use of medications, especially aspirin, nonsteroidal anti-inflammatory drugs (NSAIDs), warfarin (Coumadin), heparin, enoxaparin (Lovenox), ticlopidine (Ticlid), dipyridamole (Persantine), and clopidogrel (Plavix), not only predisposes patients to epistaxis but also makes treatment more difficult.
Hereditary hemorrhagic telangiectasia is the most common systemic disorder of the vascular system that affects the nasal mucosa. Onset of symptoms is usually at puberty and progressively worsens with age.
Blood dyscrasias can be found in patients with lymphoproliferative disorders, immunodeficiency, systemic disease, or in the alcoholic patient. Thrombocytopenia can lead to spontaneous mucous membrane bleeding, with platelet counts of 10,000/mm3 to 20,000/mm3.
Platelet deficiency can be the result of chemotherapy agents, malignancies, hypersplenism, disseminated intravascular coagulopathy (DIC), drugs, and many other disorders. Platelet dysfunction can be seen in liver failure, kidney failure, and vitamin C deficiency as well as in patients taking aspirin and NSAIDs.
von Willebrand disease is the most common clotting factor abnormality that can result in frequent, recurring nosebleeds. Factor VIII deficiency (hemophilia A) and factor IX deficiency (hemophilia B) are also common primary coagulopathies.
One study of chronic nosebleeds in children showed that a third of these patients can be expected to have a coagulation disorder. The single best predictor of coagulopathy is family history.
Because of the nasopulmonary reflex, arterial oxygen pressure will drop about 15 mm Hg after the nose is packed, which can be troublesome in a patient with heart or lung disease and often requires hospitalization and supplemental oxygen.
Tumors or other serious diseases are infrequent causes of epistaxis. However, it is prudent for all patients who present with nosebleeds to have a complete nasopharyngeal examination by an ENT specialist in follow-up.

Full access? Get Clinical Tree


