Determine the Genus and Species
Determine the family and/or genus and species of snake if at all possible. The majority of victims know not only that they were in proximity to a venomous snake, but also the snake’s common name, yet still are compelled to taunt, toy with, kiss, or otherwise handle the venomous animal for reasons that are not clear; in such patients, snake identification is not difficult. Another 25% to 30% will bring the snake to the health care facility in conditions ranging from badly mutilated to quite alive. Identification by charts or consulting herpetologists or other experts is quite useful in determining the species of the snake, whereas it is not of much benefit for the victim if he or she cannot identify the type of snake that inflicted the bite. Whether by confusion or the desire to please, children will agree that the picture of nearly any snake presented to them is indeed the offending reptile. Several online sites, such as http://www.pitt.edu/∼mcs2/herp/SoNA.html, are available to assist identification.
One can occasionally augment identification of an offending snake by the symptom complex its bite produces, as is demonstrated in Table 153.2. The prognosis is generally species dependent, but also related to the time to presentation, time to antivenom administration, the health of the host, and other factors. Management will be based on a mixture of observed and anticipated symptoms and physical findings, as well as one’s prior experience in handling this emergency.
Determine Systemic Signs and Manifestations
Assuming the patient does have signs of local envenomation, next in order is to determine whether there are any systemic signs of envenomation, remembering the fact that no one dies of local envenomation, but only from systemic manifestations. As a general rule, in mild and moderate envenomations, the symptoms are due primarily to the local pain, swelling, and discoloration, which, while quite alarming, are not usually of a life-threatening nature. Systemic symptoms such as nausea, vomiting, diarrhea, and diaphoresis, as well as fasciculations—particularly in Crotalus envenomations—do portend the possibility of a more serious outcome. Many coagulation abnormalities seen in Crotalus envenomations are often spectacular in their laboratory manifestations but systemic hemorrhage is uncommon. Altered mental status to include a noticeable stupor, and a foul metallic taste is often reported by patients with serious envenomations.
Assign Degree of Severity
In attempting to assign a degree of severity from mild to moderate to severe, one must recognize several principles. The first is that the envenomation syndrome is progressive and, secondly, evaluation is ongoing and time dependent. Two patients may be bitten to a similar degree. If the first patient is seen in 15 or 20 minutes after the bite, very few local signs of pain, swelling, or discoloration will be seen, whereas a similar patient requiring 2 hours to arrive for emergent care will report more advanced and obvious pain, swelling, and discoloration, although with exactly the same prognosis. It is the rate of change in signs, symptoms, and other manifestations that is important in grading the severity of the bite, as well as in grading the effect—or lack of effect—of the administration of antivenom.
Antivenom Administration
Because of the present lack of prospective, outcome-based studies, practices regarding perceived indications for the use of antivenom vary. Most practitioners will not administer antivenom to a patient without envenomation (“dry bites”) or to those who have only minimal envenomation, particularly if it is by the Sistrurus or Agkistrodon species. Bites by the copperhead (A. contortrix) are usually not treated (7–9) with antivenom unless the patient is at the extremes of age or with many comorbid conditions. Envenomation by the water moccasin (A. piscivorus) is notorious for a large amount of local edema but not much in the way of systemic symptoms and laboratory manifestations (10), and even less in the way of mortality. Their swelling can be so massive that, if untreated for any reason, bites of the hand may progress up the arm, chest wall, neck, face, and even abdomen; all of which is reversible.
| TABLE 153.2 Clinical Characteristics of Envenomation That Potentially Aid in Identification of Offending Pit Viper Species |
 |
| TABLE 153.3 Severity of Envenomation by Pit Vipers |
 |
Severe envenomations are often apparent by the time they arrive at the emergency department (ED), primarily because of the rapidity with which the venom initially gains entry into the circulatory system. While it is common to see someone progress from minimum envenomation to moderate envenomation, it is quite rare to see one, in our experience, progress from moderate envenomation to severe envenomation. Rather, when they arrive—even within minutes of the event—severely envenomated patients may be considerably hypotensive with lethargy, nausea, and vomiting, and require immediate and aggressive therapy (Table 153.3); suggested therapy is outlined in Table 153.4. It is useful to outline the leading edge of proximal progression of the swelling with an ink pen or felt marker. In this manner, one can observe whether the swelling is progressive or arrested. Whereas some relatively slow progression is tolerated—particularly if one elects not to treat the patient or if antivenom is not immediately available—rapid swelling, particularly with concomitant systemic symptoms, usually justifies prompt and aggressive therapy.
We do not administer antivenom in patients who have no envenomation; about 10% to 15% of people with minimal envenomation, half of those patients with moderate envenomation, and all patients with severe envenomation are administered antivenom. The offending reptiles in one’s locale and the experience of those evaluating the patient may override our simplification. Reasons for not administering antivenom to all, or nearly all, victims are several: (a) the extremely low mortality rate of envenomation by snakes native to the United States, (b) the admittedly very low rate (<0.01%) of serious and mild (14%) allergic reactions, (c) the modest rate (15%) of serum sickness–like late reactions (occurring typically 8–12 days after administration) to FabAV (1), and (d) the cost of antivenom treatment, which can easily exceed $50,000. As antivenom is more efficacious the earlier it is administered, once the decision has been made to employ the drug, it should be done promptly. Control of the envenomation syndrome is adjudged by the slowing, or preferably the cessation, of progressive local swelling (27). One should not expect extant swelling to regress or any areas of local damage to the bite site such as a swollen or discolored area to regress, as such damage has already resulted prior to the patient’s arrival and treatment. Hemorrhagic bleb formation at the site of the bite is not an important sign in and of itself, although it generates much attention; these are best left alone.
Compartment syndromes are seen rarely, and indications for surgical intervention as justified by pressure measurements in only about 1% to 2% of all envenomated patients in the United States. The degree of swelling in and of itself is not a reliable sign of compartment syndrome given the elasticity of skin. More reliable signs are total lack of function and exquisite pain of the muscles contained within a compromised compartment and, often, an intense hardness of the site owing to the nonelasticity of fascial tissue which, while limiting swelling, allows pressure to increase in tissues locked beneath the fascial plane. The palmar aspect of the hand and lateral compartment of the tibia may be so involved. Direct measurement of pressure within an anatomic compartment may be of use, yet adequate antivenom therapy and elevation will usually result in normalization of pressures. Orthopedic consultation may be indicated, but in experimental animal models, fasciotomy has not been shown to result in improved outcomes.
The mainstay for treatment for North American pit viper envenomation is ovine FabAV for bites in both adults and children (23,27). The Fab portions of sheep immunoglobulins are made by enzyme cleavage and elimination of the Fc fragment, which is regarded as the more immunogenic part of the intact immunoglobulin molecule, and by further enzymatic cleavage of the resulting F(ab′)2. Pretreatment skin or conjunctival testing is neither required nor recommended prior to the administration of FabAV. The small FabAV molecule has the theoretical advantage of a larger volume of distribution and the potential to neutralize more venom at the bite site. On the other hand, as it has a more rapid distribution and shorter half-life than intact IgG, periodic readministration during the initial treatment period is important.
| TABLE 153.4 Summary of Therapeutic Measures for Pit Viper Envenomation |
 |
Another general rule of thumb for pit viper envenomation is that approximately half of the total swelling expected to occur does so within the first 2 hours of envenomation, and nearly all of it occurs by 12 hours after envenomation. This seems congruent with one study that involved timed rate of change in swelling. Accordingly, if a patient presents over 12 hours after the bite, it would be unusual to experience significantly more swelling, and most systemic symptoms should have occurred and abated. We rarely initiate administration of antivenom treatment more than 12 hours after a bite, and essentially never after 24 hours of the bite. One may reinitiate or continue antivenom administration after 24 hours in selected situations, such as in the management of continued coagulopathic effects or in the management of recurrence syndrome.
We hold that the defibrinogenation syndrome itself is not such a clear and present risk for spontaneous hemorrhage or that its presence alone requires administration of antivenom, or that its recurrence represents an established reason to readminister antivenom (10,26). As the literature and experience garnered thus far supports that defibrinogenation alone seems benign, the administration of blood products such as fresh frozen plasma (FFP) or cryoprecipitate is usually not warranted, even prior to a surgical procedure, as the risks of these blood products probably outweigh their (unproven) benefit. If one does encounter a patient with systemic hemorrhage, or should unacceptable bleeding follow a surgical procedure, administration of additional antivenom plus cryoprecipitate (8–10 bags in an adult) is the fibrinogen source of choice (10). We advise against preemptive or prophylactic transfusion of blood products for potential or concern for bleeding reserving blood products only for actual hemorrhage and after antivenom has been administered (37).
Some species of snakes, particularly the timber rattlesnake (Crotalus horridus), have a principle in their venom that causes significant thrombocytopenia, which appears rather resistant to reversal by antivenom therapy (38). If platelet counts are significantly falling and/or are less than 10,000 to 20,000 cells/μL, administration of (additional) antivenom and infusion of platelets may be indicated, particularly if there is evidence for systemic bleeding. In general, with most Crotalid envenomation, there is a mild thrombocytopenia in the range of 50,000 to 150,000 cells/μL that is thought to be due to passive entrapment of platelets within the previously described soft fibrin network; this does not support a diagnosis of DIC.
Support
A surgical procedure for the wound is rarely indicated, and there are several case series and experimental studies suggesting that surgical procedures correlate with a delayed outcome, some with a paradoxic increase in permanent loss of tissue, loss of anatomic function, and nonspecific stiffness (37,39,40). Antibiotics are generally not employed as they are of questionable assistance, and their routine use is not recommended (37,41,42). If there has been significant surgical manipulation of the wound in the field, such as with repeated knife wounds, that stance may need to be reconsidered. Tetanus vaccination status should be ascertained as being up to date. It is best to have the extremity clearly visible so as not to compromise the evaluation; we do not advocate any covering dressings or wraps. Once the patient is at the hospital and receiving antivenom, the extremity should be elevated above the level of the heart. Monitoring is usually best performed in the ED, with subsequent admission to the intensive care unit (ICU), although ICU therapy should not be considered, in our opinion, as a necessary standard of care—the careful and frequent nursing care available in the ICU is, however. The usual length of hospitalization is 4 to 6 days. We often observe patients for up to 24 hours—either in the ED or in the hospital—who are deemed to have no envenomation or mild envenomations, and who do not receive antivenom because of the high incidence of concurrent inebriation.
Prognosis
Nearly all North American pit viper bites result in some near-instantaneous local tissue destruction, which should not be expected to be totally absent or to resolve, even with the very best and most rapid care. Most edema and swelling that does occur after antivenom treatment lasts only for a month or two, with longer recovery times seen in older or debilitated patients. In general, there is a total return of function to the bitten extremity, although some patients can experience mild stiffness, atrophy, and weakness for up to a year or more (43,44). The loss of tissue, including fingers or limbs, is very rare, and often occurs with the injudicious prehospital use of ice or tourniquets or, perhaps, very delayed care. Unfortunately, patients who are bitten by snakes tend to continue their risky behavior, resulting in the finding that reenvenomation is not rare.
SNAKES NOT NATIVE TO THE UNITED STATES
This section summarizes the epidemiology, pathophysiology, diagnosis, and treatment of nonnative snake envenomations in the United States. Envenomations by reptile, amphibian, arthropod, or marine species not native to the United States pose special challenges to the clinician as they are likely to be unfamiliar with the clinical spectrum of exotic envenomation and its current management. Antivenoms, if they exist, may not be available or may take many hours to locate and deliver to the location of the envenomated patient. Zoos, aquaria, and academic institutions may obtain and stock antivenoms to non-native animals in their possession for potential treatment of their workers. The problem is compounded by private collections, whose existence is not usually known to their regional health care system until an exposure occurs and whose keepers are unlikely to possess the appropriate antivenoms. Policies and procedures governing acquisition, storage, handling, antivenom, and preparations for managing envenomations range from comprehensive to nonexistent.
The severity and spectrum of effects in envenomation varies widely. A significant number of bites and stings do not result in envenomation. However, life-threatening effects may be seen and fatalities in venomous snakebite occur at a much higher rate than for native envenomations, because of the inherent toxicity of non-native species, difficulties and delays in obtaining appropriate antivenom and clinical unfamiliarity with management of these envenomations. Identification to the species level of the envenomating organism is important in anticipation of effects and the selection of nonspecific and specific therapies. Therapies other than antivenom may be available, and nonspecific therapies are directed at general classes of venom effects.
Epidemiology
There are about 3,000 snake species in the world, of which fewer than 300 are dangerous to humans (45). Venomous reptiles include the families Atractaspididae, Colubridae, Crotalidae, Elapidae, Hydrophiidae, and Helodermatidae (45). Between 40 and 50 nonnative snake envenomations occur per year in the United States. Although nonnative envenomations in the United States involved dozens of species over the past 20 years (46,47), certain families, genera, and species are more commonly encountered. Cobras (family Elapidae) account for one-third of all nonnative venomous snake exposures, and 86% of Elapid envenomations. Viperids account for 46% of all nonnative venomous snake exposures, with Bothrops, Bitis, and Lachesis genera accounting for the 53% of all Viperid envenomations (46,47).
Compared with other etiologies of critical illness, venomous snakebites account for few ICU admissions per year. Nevertheless, almost one-third of nonnative envenomations develop major to moderate symptoms and signs of disease, and are admitted to an ICU. The case fatality rate of approximately 1% is significantly greater than in native snakebites. Males are involved in 84% of bites, a similar percentage to that in native bites. Almost 15% are aged 17 years or less, and approximately 7% are aged 5 years or younger, most likely as a result of private collections in home settings (47). Identification of the snake in nonnative bites is usually not difficult, as zoos, aquaria, and academic institutions will know their collections to the species or subspecies level and have procedures in place to identify the biting snake. The private collector is also usually well informed. However, the bitten individual with a private collection may not be capable of communication, and potential penalties for possession of venomous animals in some jurisdictions may result in the withholding of critical information (48). A qualified herpetologist should be consulted for the identification of nonnative snakes that are otherwise unidentified. The presence of a puncture and typical appearance of the site, progression of findings, and consistent laboratory abnormalities of a snakebite indicate the possibility even when the history is not available.
Pathophysiology
The venom glands of poisonous snakes are modifications of salivary glands (49). The venom of a single snake is a complex mixture of enzymes, nonenzymatic proteins and peptides, and other substances (50,51). These substances exert simultaneous toxic or lethal effects on the integumentary, hematologic, nervous, respiratory, muscular, and cardiovascular systems. The clinical picture also can be complicated by the effects of endogenous mediator release, such as histamine, cytokines, and nitric oxide (52). Some of these components may be found in all venomous snakes, with mixed clinical effects. The most important deleterious components of snake venom are shown in Table 153.5. Hyaluronidase is found in all venoms and produces hydrolysis of connective tissue stroma, allowing the dispersion of other toxic components (53). Zinc-dependent metalloprotease enzymes damage vascular membranes and produce local and systemic hemorrhage (54,55). Phospholipases are found in most snake venoms, with a variety of effects (50), including destabilizing biologic membranes and abolishing the selective membrane ion channel permeability to ions such as calcium (56,57). Crotalid venom is rich in proteinases, amino acidases, and phospholipases, and typically produces findings of cellular destruction, increased membrane permeability, and coagulation impairment. Coagulation abnormalities may result from multiple mechanisms, including consumption, aggregation or inhibition of platelets, or effects on the coagulation cascade, such as activation or inhibition of coagulation factors, procoagulant activity, defibrinogenation, prothrombin action, collagenase-like activity, and other effects (16,58,59). Elapid venoms vary widely among species but contain more neurotoxins and cardiotoxins (51), resulting in various expressions of neurologic and cardiac toxicity; sea snakes have venom similar to elapids.
Diagnosis and Monitoring
The spectrum of symptoms and signs produced in a victim by a given venomous snakebite varies with the species of snake, the natural variability in venom composition between snakes, and, in any given snake over time, the quantity of venom injected, bite location, and the age and health of the victim.
Size and Species
In general, larger snakes contain and deliver more venom, but fatal envenomations may result from small species and juvenile snakes. Toxicities of the venom will depend on the species and other factors that affect venom production.
Quantity Injected
As many as 30% of Crotalid bites and 50% of Elapid bites may result in no envenomation (60). When venom is injected, the amount may be reduced by poor penetration of the fang or high tissue pressures, as in fingertips. The volume of available venom may also be reduced by recent previous feedings.
| TABLE 153.5 Some Components of Snake Venom |
 |
Bite Location
Tissues and anatomic areas with a low capacity for swelling, or which are functionally important, such as the fingers or hand, are particularly at risk of both short- and long-term impairment. The destructive effects of proteolytic enzymes may directly damage tissues. Also, even where no true compartments exist, tissue pressures may be significantly elevated and vascular compromise may occur. True muscle compartments may be subject to elevated pressures, either because of direct injection of venom with intracompartmental edema, from passage of venom into a compartment via direct spread or lymphatics, or as a result of extrinsic pressure on a compartment secondary to subcutaneous edema. Lower extremity bites may accumulate enough edema fluid to affect hemodynamic stability, particularly in children. They may also damage venous valves and produce long-term dependent edema. Decreased mobility and mobilization after a bite may predispose to deep venous thrombosis or other morbidities. Upper extremity, torso or head and neck bites may result in airway compromise secondary to edema.
Age and Health of the Victim
Those at greatest risk of morbidity and mortality include patients with long delays to treatment, those with significant comorbid conditions, and those at the extremes of age. Because of smaller body mass, children receive a relatively greater dose of venom. As with native envenomations, some private collectors may be under the influence of alcohol at the time of envenomation, which may affect their ability to avoid envenomation, predispose to multiple bites, and delay seeking care.
Symptoms and Manifestations
Since various factors may affect the quantity and specific components available and delivered, it is difficult to make an a priori determination of the clinical potential of the envenomation. The manifestations of snake envenomations can be divided into local and systemic effects.
Local Effects
Snake venom that produces local effects causes pain and edema at the bite site, erythema, ecchymosis, and occasional bleb formation. Later, the increased membrane permeability and cellular destruction produced by proteases result in spreading edema both distally and proximally, and may cause tissue necrosis. If the bite is on an extremity, elevated tissue pressures may compromise vascular supply or result in elevated compartmental pressures. Periodically marking—with an ink pen or felt marker—the extent over time of proximal spread of edema directly on the skin is useful in documenting the progression of local venom effects and response to treatment. The leading edge is usually palpable as a sharply demarcated ridge and differs from later redistribution of tissue edema, which more gradually transitions to normal tissue. Edema may spread from an extremity onto the trunk or involve the head and neck, compromising the airway (61,62). Pain, possibly requiring opioid-level management, is common and cannot be used to diagnose compartment syndrome. Because of the similarity of findings with compartment syndrome, if there is concern for elevated tissue or compartmental pressures, they should be measured directly (Stryker Intra-Compartmental Pressure Monitor System, Stryker United Kingdom; COACH Transducer, MIPM GmbH, Mammendorf, Germany). Local venom effects will respond to adequate amounts of antivenom with cessation of progression of proximal edema and reduced tissue pressures. Recurrence of progression of local effects may occur, particularly with Fab antivenoms, which have a larger volume of distribution and, thus, its circulating concentrations fall more quickly than F(ab′)2 or IgG antivenoms. Locally acting venom components are usually exhausted by 24 to 36 hours, although the resulting tissue injury may continue to develop over days to weeks. Starting on the second day post envenomation, the clinical appearance of the bitten extremity, with increased heat and inflammation of the lymphatics, may be difficult to distinguish from an infective process. Overall, the incidence of infection is low, but will vary depending on the snake, the host, and factors such as the development of necrosis and wound manipulation. Potentially life-threatening infections such as necrotizing fasciitis and disseminated osteomyelitis have been reported following snakebites (63–65).
Hematologic Effects
Coagulation alterations result from proteases acting on various parts of the coagulation cascade and may occur singly or in any combination. Fibrinogenolysis may occur, resulting in decreased levels of fibrinogen and increased levels of FDPs (16,65–68). Platelet inhibition, aggregation, or consumption may occur with abnormal function and/or decreased platelet counts (16,69). Intravascular hemolysis has also been reported with some snake venoms (70). The coagulation defects may result in local or systemic bleeding, including life-threatening hemorrhage as well as thrombotic events (70–75). Laboratory tests, including a complete blood count (CBC) with platelet count, PT/international normalized ratio (INR), PTT and fibrinogen, should be obtained on arrival and periodically reassessed. A single d-dimer (or fibrinogen degradation product) test should be be obtained at least two hours post bite to assess whether fibrinogen destruction is occurring. Regardless of whether frank hypofibrinogenemia develops during hospitalization, patients with an elevated d-dimer are at risk of recurrent or delayed coagulopathy. Most patients who will develop hematologic abnormalities will demonstrate them within 1 to 2 hours, although early use of antivenom may mask this finding; normal hematologic values at 6 hours suggest an absence of such effects. If abnormalities are present, the use of antivenom may halt (e.g., fibrinogenolysis) or reverse (e.g., platelet aggregation) venom effects. The timing of repeat labs is based on the use of antivenom, clinical findings, and laboratory trends. Unneutralized venom components responsible for hematologic effects may remain active in the body for up to 3 weeks, resulting in delayed, persistent, or recurrent hematologic abnormalities (29,76,77).
Neurologic Effects
These may result from Atractaspid, Elapid, Helodermid, Hydrophiid, or Viperid envenomations. Clinical effects can include sweating, numbness, paresthesias, convulsions, coma, muscle fasciculation, muscle weakness, and respiratory arrest. Respiratory muscle paralysis is the primary cause of death with most Elapid and Hydrophiid venoms. Viperid snakes rarely cause clinically significant respiratory compromise. Coma may be secondary to hypovolemia or to a direct effect of the toxin (67). Neurologic effects may develop rapidly, with respiratory arrest occurring within 15 to 30 minutes, but also may be delayed by many hours (78,79). Measures such as the application of a PIB may also delay the onset of neurotoxicity (80). Even with delayed onset, once neurologic effects occur, they may progress very rapidly. Patients should be observed for a sufficient period of time, and preparations to manage the airway should be readily available. It should be kept in mind that some Elapids produce little to no local effects, and therefore, their absence cannot be relied upon to confirm nonenvenomation. Once muscle weakness or paralysis has occurred, it may be difficult to reverse, although both antivenom and cholinergic agonists will generally stop the progression of effects and have been reported to result in either dramatic or more rapid improvement than would otherwise be expected (81–83). Extubation criteria are based on standard tests of respiratory sufficiency.
Nonhematologic Systemic Effects
These include effects on the cardiovascular, respiratory, and neurologic systems. In general, snakes from any family may produce any of these effects, although certain effects predominate within families. Type I hypersensitivity reactions to venom (IgE or non-IgE mediated) with or without hypotension may occur; the incidence is believed to be approximately 1% (84). Type I hypersensitivity reactions are characterized by wheezing, urticaria, laryngeal edema, and/or hypotension. Airway compromise from laryngeal edema may also occur, and direct myocardial depression, injury, or dysrhythmic effects of venom have been reported (84–89). The clinical picture may be complicated by possible adverse reactions to antivenom. The incidence of type I hypersensitivity to antivenoms varies from less than 5% to 25%. Other systemic findings common in snakebites are nausea, vomiting, diaphoresis, and pulmonary edema, especially in more severe cases. These usually resolve in response to antivenom and rarely persist beyond the immediate postbite period. Adverse reactions to antivenoms can complicate care. Type III hypersensitivity reactions—“serum sickness”—may occur in any patient who has received antivenom and are the result of circulating immune complexes. The frequency of occurrence is dependent on the amount of antivenom received as well as the type (e.g., source animal, immunoglobulin fragment). Type III reactions usually occur between 5 and 21 days after receiving antivenom and vary widely in incidence by antivenom utilized, from less than 5% to 100% (90–94). Symptoms and signs usually consist of muscle and joint aches, low-grade fever, and/or an urticarial rash; severe cases may have severe symptoms, including renal insufficiency.
Diagnosis
The diagnosis of snakebite may be a clinical one and should be suspected in any unknown presentation with any of the above clinical manifestations. Although immunoassays and bioassays have been used to identify various snake venoms in tissue within endemic areas, such tests are not available in the United States (95,96). In the United States, envenomations are likely to occur in zoo, academic, and private collector settings (47). Snake identification may be inaccurate in noninstitutional settings, yet obtaining an accurate identification of the snake is of utmost importance in order to select the appropriate antivenom. When dealing with private collectors, consideration should be given to independently verifying the snake species. A local zoo or aquarium may be of assistance in identifying the snake.
| TABLE 153.6 Prehospital Management of Snakebites |
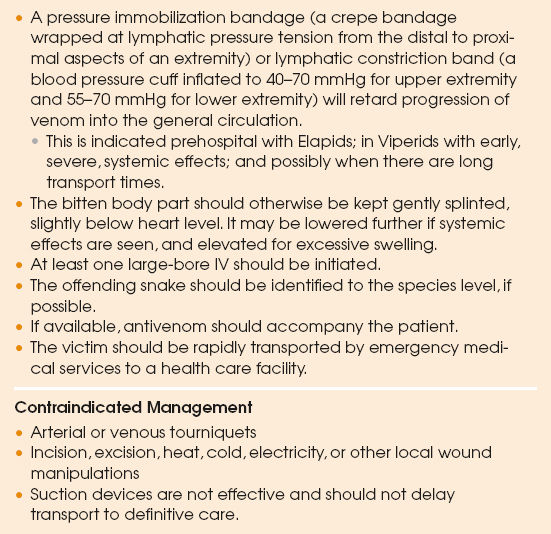 |
Management
The management of clinically significant snake envenomation can be divided into first aid, specific antivenin therapy, and supportive therapy (Table 153.6).
Online Antivenom Index
Initiation of efforts to obtain the appropriate antivenom should not wait until symptoms or signs develop; rather, this should be done immediately following the bite. The Online Antivenom Index is a resource for determining the appropriate antivenom(s) for any given snake and maintains a continuously updated listing of zoo antivenom stocks and contact information. It is accessible by regional poison centers (1–800–222–1222), which can assist in the identification and acquisition of an appropriate antivenom and in the clinical management of a snake envenomation.
First Aid
In general, the patient should get away from the snake and the snake should be secured by a qualified individual. Pre-existing medical information, information regarding the biting species, and any available antivenom should be transported with the patient. The bitten body part should be splinted to slow the passage of venom into circulation (97). With envenomations from known neurotoxic snakes, generally the Elapids and sea snakes, the application of a PIB (a wide crepe bandage wrapping the entire extremity from distal to proximal at lymphatic compression pressures) or an LCB (i.e., a blood pressure cuff inflated to 40–70 mmHg for upper extremity and 55–70 mmHg for lower extremity envenomations) has been shown to slow central compartment spread of venom and reduce the risk of out-of-hospital respiratory arrest, and thus should be routinely employed (98,99). With Viperid envenomations, the risk of rapidly developing life-threatening systemic effects is generally less. Although the use of a PIB prolonged survival in an animal model, it also resulted in increased tissue pressures; thus, the potential benefits must be weighed against the risk of increased local injury in Viperid envenomations (100). Hypotension, airway compromise, or other signs of a severe type I hypersensitivity reaction would be examples of appropriate indications for the use of a PIB or LCB in a Viperid bite. In general, prior to arrival at a hospital and administration of antivenom, the bitten area should be kept at or slightly below the level of the heart. A dependent position may be used if rapid, severe systemic effects are occurring. These measures can be instituted on arrival at the hospital if they have not been done previously. Transport to a health care facility should be by paramedic ambulance. The initiation of two, large-bore intravenous lines is a sensible precaution. The PIB or LCB should not be removed until antivenom has been obtained and is infusing, if nonenvenomation appears to be the case, or a decision has been made to observe the patient without specific treatment (Table 153.7).
| TABLE 153.7 Hospital Snakebite Site and Wound Management |
 |
Hospital Care
At the hospital, basic wound care should be provided, including updating the tetanus status, if needed. If, after a sufficient period of observation, which varies from 8 to 24 hours depending on the species of the snake, the victim demonstrates no signs or symptoms of envenomation, the person can be released from the hospital (Tables 153.7 to 153.9).
Pain Control
Opioid analgesics are best deferred until after hospital evaluation because of the risk of potentiating respiratory depression. An ice pack applied to the bite site, with customary precautions, may provide some pain relief without risking additional tissue injury (97,101). Opioid-level analgesia, however, may be required and its judicious use can be considered.
| TABLE 153.8 Hospital Snakebite Antivenom Management |
 |
| TABLE 153.9 Hospital Snake Bike Symptom Management |
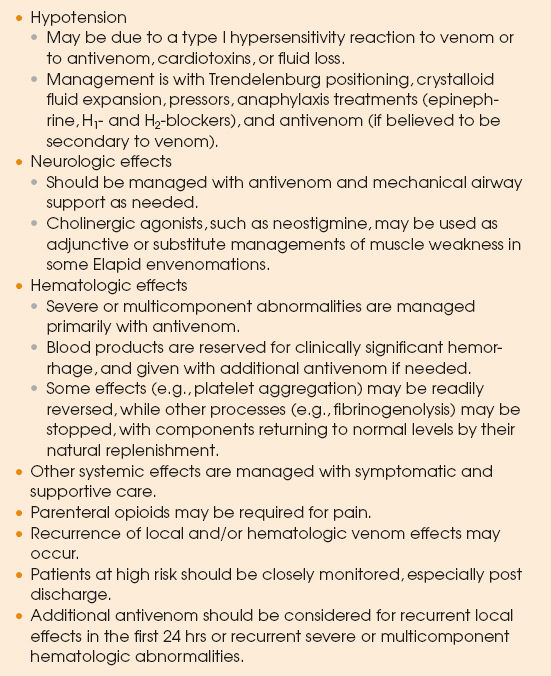 |
Antibiotics
Most authors recommend against routine prophylactic antibiotics. Antibiotics are suggested only for those with necrosis or clinical or laboratory evidence of infection (102).
Antivenom
Antivenom is composed of antibodies raised in an animal such as a sheep or horse to the venom of one or more species of snakes. A single snake’s venom may be used to produce a monovalent antivenom, effective only against that snake or other snakes with the same or a subset of venom components. Since, in their endemic areas, it may not always be possible to identify the biting species, many antivenoms are polyvalent; that is, they are designed to provide neutralizing efficacy for a number of different snake species. Venoms range from those that are relatively unpurified—whole IgG immunoglobulins, containing other proteins and immunoglobulin fractions—to highly purified specific IgG, F(ab′)2, or Fab immunoglobulin fragments. In general, horse serum–based products are more immunogenic than sheep-based antivenoms. IgG has a smaller volume of distribution, longer half-life, and higher rates of type I and type III hypersensitivity reactions, while Fab antivenoms have the largest volume of distribution, shortest half-lives, and lowest rates of allergic reactions. There is both considerable overlap and considerable variation of venom components within genera and species. When possible, species-specific antivenom that claims efficacy for the particular snake should be used. Antivenoms effective against other snakes in the same genus may be tried if species-specific antivenom is not available.
Antivenoms for nonnative snakes are imported into the United States under Investigational New Drug (IND) application. As such, their use carries additional Food and Drug Administration (FDA) and institutional review board (IRB) reporting requirements. As no US hospital routinely stocks antivenoms for nonnative species, such antivenoms are generally acquired by zoos and other institutions against the species they have in their collection for use in the event of one of their workers being envenomated. Zoos have traditionally made their antivenoms available to physicians on a compassionate basis. Since an IND antivenom will usually be brought into a hospital from an outside, nonhospital source, questions may be raised by the pharmacy regarding storage conditions, expiration dates, and other issues relating to its administration. If the potential for a nonnative envenomation can be anticipated, such as a known zoo or university collection, it is prudent to have an existing protocol as well as having obtained prior IRB approval (103).
Antivenom is considered the definitive treatment for all clinical effects of snake venom, although for a variety of reasons, such as incorrect snake identification, geographic variation of venom components, irreversible or time-dependent toxicity, and so forth, it may have limited to no observable efficacy against any particular venom effect (104–107). In addition, there are rarely prospective, controlled clinical trials to document appropriate indications, efficacy, and safety or to establish optimal dose and dosing regimens. Since antivenoms carry a risk of allergic reactions, potential benefits must be weighed against the risks of administration. Skin tests are neither sensitive nor specific enough to predict type I hypersensitivity reactions and their use is discouraged. If performed, however, the result should not serve as a contraindication to administration when indicated, and preparations to manage an allergic reaction should always be immediately available. Some antivenoms with known high rates of adverse reactions may routinely be recommended to co-administer with epinephrine or other medications. Expert guidance is suggested. Regardless, skin testing should not delay administration of antivenom in a life-threatening envenomation.
Treatment with antivenom alters venom component distribution pharmacokinetics. Venom components bound to antibody become inaccessible to target tissues and are thus neutralized. Therefore, the dose of antivenom should be great enough to theoretically bind/neutralize the entire venom dose injected by the snake. These doses have been determined by knowledge of typical snake venom loads, neutralization properties of antivenoms in animal studies, and clinical studies. In most cases, it would be best to give doses of antivenom to ensure adequate venom neutralization on the assumption of a severe envenomation, since the degree of envenomation is difficult to appreciate early in the course. Such neutralization, however, occurs predominantly in the vascular compartment, and there may be unneutralized venom components remaining in the tissues. Venom may thus redistribute from target tissues and continue to produce toxicity if the antivenom dose is inadequate or if unbound antivenom has been eliminated. These pharmacokinetic relationships illustrate why antivenom administration as soon as possible following envenomation is beneficial and why the use of shorter-acting antivenoms may result in recurrent hematologic effects. Also, because of difficulty reaching damaged tissue and despite the use of antivenom early in the course of a snake envenomation, there may still be limitations as to the effectiveness of antivenom in preventing worsening of local tissue damage, and it will not benefit already devitalized tissue.
Indications, timing, and doses of antivenom will vary and expert guidance should be sought. Since the required dose of antivenom is that needed to neutralize a given amount of venom in the body, it is not dosed by patient weight, and children may require larger doses than adults. Over a 10-year period in the United States, antivenom was only used in 26% of nonnative snake envenomations, possibly because of difficulties in determining, locating, and obtaining appropriate antivenom in a timely manner (47,103). Antivenom is most effective in preventing or ameliorating local venom effects when given early in the course. Since most local reactions have stopped progressing within 24 to 36 hours, giving an initial dose of antivenom after this time frame is not likely to be of any benefit. Antivenom is also most effective at preventing or reversing hematologic effects when given early, but may still be beneficial for weeks after an envenomation if there are still circulating venom components (66,76,108). Clinically significant hemorrhage is managed with additional antivenom as well as blood component therapy. Large doses may be required to stop or reverse some effects.
Finally, zoos may only have or choose to send expired antivenom. Expired antivenoms may have decreased efficacy and thus may require higher doses, but barring discoloration or frank contamination, there is otherwise no contraindication to their use. The regional poison center should be contacted for further assistance (1–800–222–1222).
Surgical Management
Frankly devitalized tissue, usually becoming evident several days following an envenomation, should be debrided. Because high concentrations of venom have been found in blisters overlying the bite area, unroofing these should be considered. Fasciotomy or dermotomy have been advocated for compartment syndrome or tense tissue edema potentially affecting blood flow. Unfortunately, a true compartment syndrome is difficult to diagnose by clinical means, since the typical signs and symptoms of snake envenomation mimic classic compartment syndrome findings, and early surgical intervention often leads to prolonged convalescence, increased tissue damage, decreased function, and greater scarring. Finally, there is no evidence of improved outcome, and there is animal-model evidence of increased myotoxicity with fasciotomy (109). Reported fasciotomy rates vary by geographic region and historical practice, ranging from 0% to greater than 10%. Fasciotomy should only be considered in patients with objective evidence of a compartment syndrome (i.e., a documented significant increase in intracompartmental pressures), vascular impairment, unusual entrapment syndromes, or other tissue threats that are unresponsive to an adequate trial of antivenom and elevation (110–114). Mannitol and hyperbaric oxygen have also been used in conjunction with antivenom (115); noninvasive vascular studies may identify patients at risk for ischemia (116) and ultrasound may help to establish the location of edema (116a).
Other Supportive Therapies
These include basic wound care and updating tetanus status. Blood products should be reserved for significant hemorrhage or hemolysis and administered with additional antivenom. Ventilatory support and hemodialysis may be necessary for pulmonary and renal complications of severe envenomation. Corticosteroids may be used for hypersensitivity reactions to venom or antivenom. Antibiotics are indicated for documented infection or in the presence of frank necrosis.
Hypersensitivity Reactions
If a type I hypersensitivity reaction develops, the antivenom infusion should be stopped. Anaphylactoid reactions are primarily related to rate of infusion, and stopping the infusion often results in rapid improvement. Anaphylactic reactions (i.e., those IgE mediated) are often dramatic and continue to progress after the infusion has been stopped. There is, as one might expect, considerable clinical overlap between the reactions (117). Standard managements should be used. If symptoms persist, the patient should be treated with H1-blockers (e.g., diphenhydramine, 50 mg IV) and H2-blockers (e.g., ranitidine, 50 mg IV). Wheezing may respond to β-adrenergics by nebulizer (e.g., albuterol). If there is hypotension or laryngeal edema, epinephrine, either subcutaneously or intravenously, should be considered (118). Antivenom should be withheld until the reaction has subsided and then a determination made whether to restart it. If restarted, the patient should receive pretreatment with H1– and H2-blockers and the infusion begun more slowly.
Type III reactions are usually managed with nonsteroidal anti-inflammatory drugs (NSAIDs) and H1– and H2-blockers. More severe cases may require opioid-level pain relief, as well as corticosteroids. All patients receiving antivenom should be cautioned regarding the possibility of a type III reaction occurring after discharge.
Postdischarge Considerations
It is desirable to see patients at least once after discharge to monitor for persistent or recurrent hematologic effects, if indicated, or tissue injury and its sequelae, and to refer for physical or occupational therapy in order to maximize functional recovery. Patients treated with a Fab antivenom may need monitoring for more than a week to detect and manage possible late coagulopathy. Patients should also be cautioned about the possible risk of sensitization to snake venoms or antivenoms regarding possible future envenomations (Table 153.10).
Nonrecommended Treatment
Some treatments are ineffective or dangerous and are therefore not recommended.
| TABLE 153.10 Postdischarge Management Following Snakebite |
 |







Full access? Get Clinical Tree


