![]() Penetrating Chest Trauma
Penetrating Chest Trauma
![]() Traumatic arrest with witnessed signs of life* in the field
Traumatic arrest with witnessed signs of life* in the field
![]() Persistent hypotension (systolic blood pressure (SBP) <60 mm Hg) despite resuscitative efforts
Persistent hypotension (systolic blood pressure (SBP) <60 mm Hg) despite resuscitative efforts
![]() Blunt Trauma
Blunt Trauma
![]() Traumatic arrest that occurs in the emergency department (ED)
Traumatic arrest that occurs in the emergency department (ED)
![]() Persistent hypotension (SBP <60 mm Hg) despite resuscitative efforts
Persistent hypotension (SBP <60 mm Hg) despite resuscitative efforts
![]() Pulmonary Trauma
Pulmonary Trauma
![]() Chest tube drainage >1,500 mL
Chest tube drainage >1,500 mL
![]() Persistent hypotension or cardiac arrest with known lung laceration
Persistent hypotension or cardiac arrest with known lung laceration
![]() Air Embolism
Air Embolism
![]() Persistent signs of hypovolemic shock
Persistent signs of hypovolemic shock
![]() Hemoptysis and cardiac arrest after intubation and ventilation
Hemoptysis and cardiac arrest after intubation and ventilation
![]() Nontraumatic Hypothermic Cardiac Arrest
Nontraumatic Hypothermic Cardiac Arrest
![]() In settings where cardiopulmonary bypass is not immediately available
In settings where cardiopulmonary bypass is not immediately available
![]() Goals
Goals
![]() Relief of cardiac tamponade
Relief of cardiac tamponade
![]() Support of cardiac function with open massage, cross-clamping the aorta, and/or internal cardiac defibrillation
Support of cardiac function with open massage, cross-clamping the aorta, and/or internal cardiac defibrillation
![]() Control of hemorrhage
Control of hemorrhage
![]() Diagnosis and management of air embolism
Diagnosis and management of air embolism
![]() Mediastinal irrigation and rewarming (for hypothermic cardiac arrest)
Mediastinal irrigation and rewarming (for hypothermic cardiac arrest)
CONTRAINDICATIONS
![]() No signs of life and prehospital cardiopulmonary resuscitation (CPR) performed:
No signs of life and prehospital cardiopulmonary resuscitation (CPR) performed:
![]() >15 minutes after penetrating trauma
>15 minutes after penetrating trauma
![]() >10 minutes after blunt trauma
>10 minutes after blunt trauma
![]() Multisystem blunt trauma
Multisystem blunt trauma
![]() Severe head injury
Severe head injury
![]() Asystole as an initial rhythm without tamponade
Asystole as an initial rhythm without tamponade
![]() Inability to provide definitive care after procedure
Inability to provide definitive care after procedure
RISKS/CONSENT ISSUES
![]() This is an emergent procedure and does not require written consent
This is an emergent procedure and does not require written consent
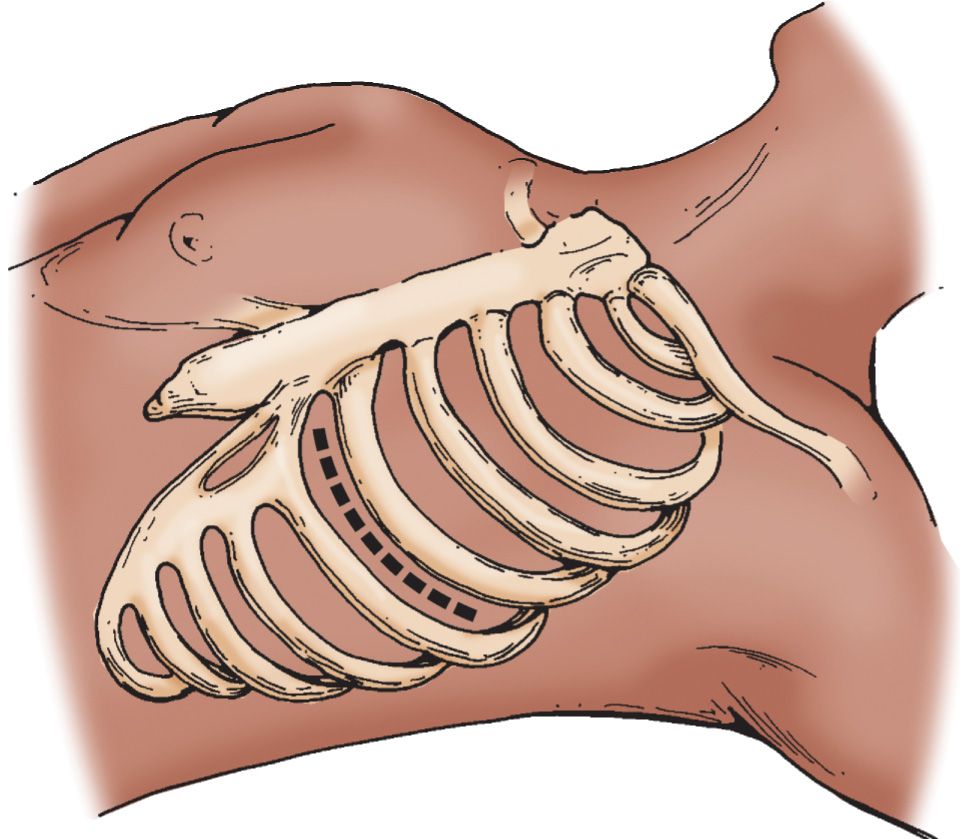
LANDMARKS (FIGURE 15.1)
![]() Left-sided supine anterolateral approach over the 5th rib, in the fourth intercostal space
Left-sided supine anterolateral approach over the 5th rib, in the fourth intercostal space
![]() In males incise below the nipple
In males incise below the nipple
![]() In females below the inframammary fold
In females below the inframammary fold
![]() General Basic Steps
General Basic Steps
![]() Incision
Incision
![]() Dissection and rib spreading
Dissection and rib spreading
![]() Pericardotomy
Pericardotomy
![]() Cardiac massage
Cardiac massage
![]() Hemorrhage control
Hemorrhage control
![]() Aortic cross-clamping
Aortic cross-clamping
TECHNIQUE
![]() Patient Preparation
Patient Preparation
![]() Patient should be intubated and a nasogastric tube should be placed (this should not delay the procedure!)
Patient should be intubated and a nasogastric tube should be placed (this should not delay the procedure!)
![]() Place towels under the left chest and place left arm above the head
Place towels under the left chest and place left arm above the head
![]() Sterilize the incision area with copious povidone–iodine solution
Sterilize the incision area with copious povidone–iodine solution
![]() Incision
Incision
![]() Using a no. 20 blade, incise from the sternal border to the posterior axillary line
Using a no. 20 blade, incise from the sternal border to the posterior axillary line
![]() During the primary incision, cut firmly through subcutaneous tissue to the intercostal muscle
During the primary incision, cut firmly through subcutaneous tissue to the intercostal muscle
![]() Dissection and Rib Spreading
Dissection and Rib Spreading
![]() Using scissors, cut the intercostal muscles above the 5th rib to avoid the neurovascular bundle
Using scissors, cut the intercostal muscles above the 5th rib to avoid the neurovascular bundle
![]() Temporarily stop ventilation just before exposing the pleura to avoid lacerating the lung
Temporarily stop ventilation just before exposing the pleura to avoid lacerating the lung
![]() Insert rib spreader with the ratchet placed toward the axilla and handlebar down
Insert rib spreader with the ratchet placed toward the axilla and handlebar down
![]() Use a Gigli saw, Lebsche knife, or trauma shears to cut the sternum for right-sided exposure
Use a Gigli saw, Lebsche knife, or trauma shears to cut the sternum for right-sided exposure
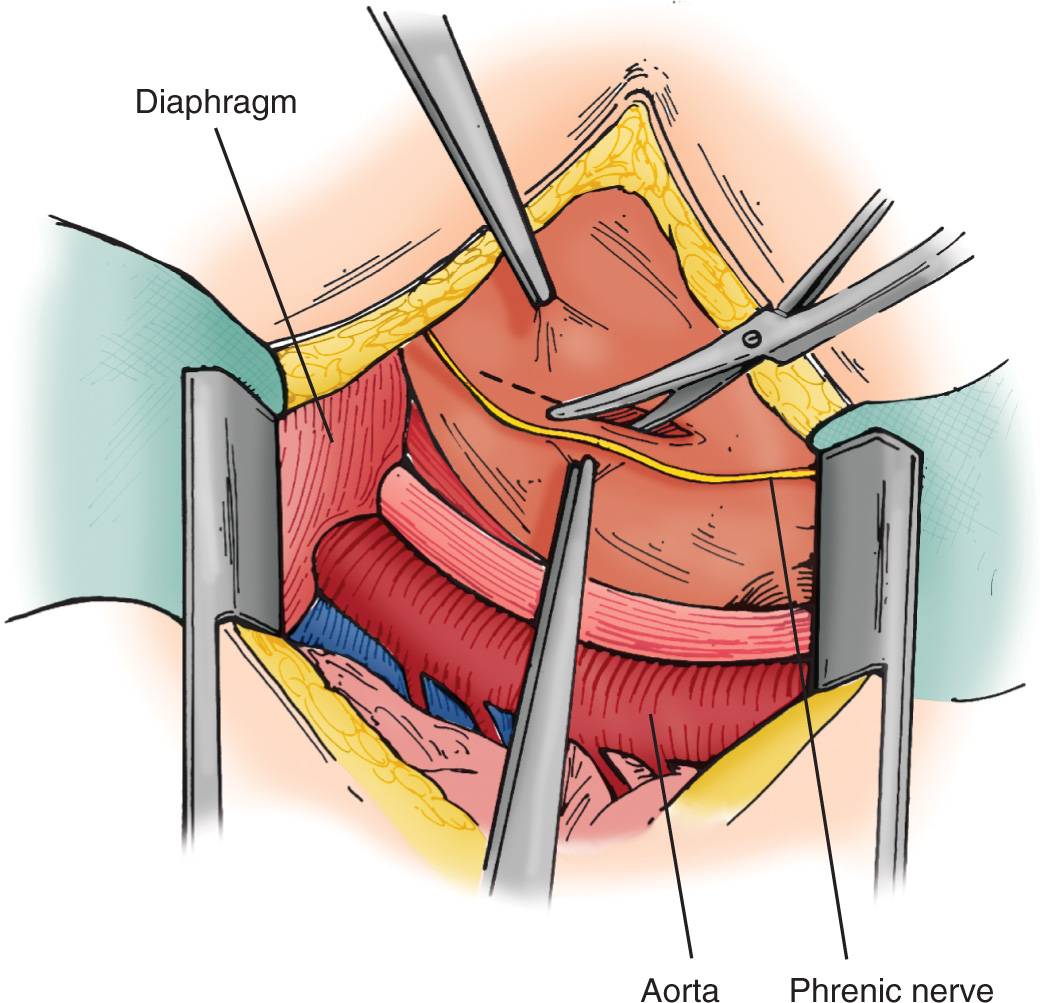
![]() Pericardiotomy
Pericardiotomy
![]() Hold the pericardium with forceps, and use scissors to cut from the cardiac apex to the aortic root (FIGURE 15.2)
Hold the pericardium with forceps, and use scissors to cut from the cardiac apex to the aortic root (FIGURE 15.2)
![]() The incision should be made anterior and lateral, avoiding the left phrenic nerve
The incision should be made anterior and lateral, avoiding the left phrenic nerve
![]() Evacuate blood and clots from the pericardium
Evacuate blood and clots from the pericardium
![]() Deliver the heart from the pericardium if cardiac repair is required
Deliver the heart from the pericardium if cardiac repair is required

Full access? Get Clinical Tree


