Chapter 23 Electrical hazards and their prevention
Mains electricity supply
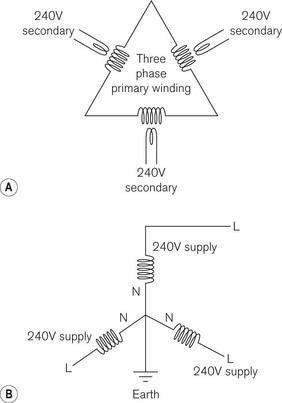
In cables carrying DC, one cable is designated positive and the other negative, which is not the case with AC cables. Fig. 23.1A shows how a three phase, 16 kV primary winding of a substation transformer steps the voltage down to a three phase 240 V root-mean-square supply (325 V peak). It also shows how these secondary 240 V windings are linked together and connected to earth at the ‘star point’ (Fig. 23.1B). For each 240 V supply, therefore, one end is deemed ‘live’ and the end connected to earth at the star point is deemed ‘neutral’.
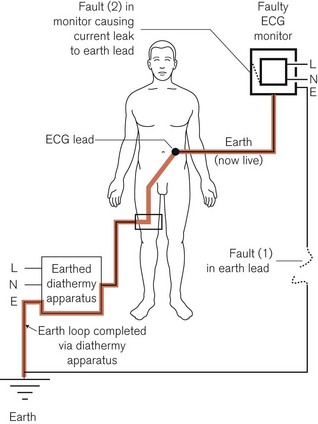
Because of this earthing of the neutral conductor at the power station, any person or object who is also connected to earth would complete an electric circuit by touching the live conductor, even if no contact were made with the neutral one. Fig. 23.2 shows how, under certain conditions, the circuit connecting a patient to a live lead may be completed by, for example, an earthed diathermy plate, resulting in fatal electrocution. However, in most modern diathermy machines, this plate is isolated from earth as far as mains current is concerned (see Chapter 24). Furthermore, here in this example of a faulty monitor, an additional interruption of the neutral cable would result in the apparatus not working. However, because the live cable is still functioning, any contact with the (‘live’) casing would lead to electrocution of an inadvertently earthed user.
Stringent precautions should be taken to ensure that the polarities are correctly defined and connected for all mains electrical apparatus. Electrical accidents can be minimized by careful, regular maintenance by qualified personnel. It cannot be overemphasized that, if a fault exists, the apparatus should be removed from use and the services of a competent technician sought. The current international standard regulating electromedical equipment, IEC 60601-1, lays down quite specific testing regimens for electromedical equipment before use.1,2
The inclusion of a lead which connects the metal chassis, frame and enclosure of the apparatus to earth ensures that under faulty conditions the enclosure is prevented from becoming live, and is thus called the ‘earth’ lead. The faults in Fig. 23.2 show a break in the earth lead to the metal enclosure of the monitor (1); this allows a second fault within the monitor (2) to render the apparatus dangerous to the patient. This is discussed further in the section below, on Class I equipment.
Apparatus can be rendered safer by the inclusion of a fuse in the electrical circuit. This may be installed in the mains supply circuit, in the plug of the electrical lead to the apparatus, or in the apparatus itself. It usually consists of a fine gauge wire, which melts if the current passing through exceeds that against which they are intended to offer protection. So, in Fig. 23.2, if the earth lead of the monitor were intact, the fault consisting of a current leak between the apparatus and its enclosure, assuming adequate leakage current and low enough fuse rating, would result in a fuse in the live wire melting, breaking the continuity of the electrical circuit and the apparatus being rendered harmless. However, there is a risk that the fuse may not protect against electric shock. This can happen if someone is in contact with the equipment as the fault develops and before the fuse has time to melt (see below). Fuses are used mainly to interrupt the electric supply in the event that the current passing through the equipment exceeds a predetermined level that might cause overheating or damage. Other types of safety devices are mentioned later in the chapter.
Pathophysiological effects of electricity
The pathophysiological effects of electric current passing through the human body include:
• resistive heating of the tissue and thermal burns
• electrical stimulation of excitable tissues, such as respiratory muscles and the heart
• electrochemical effects (electrolysis), when DC can cause chemical burns
The body may be considered electrically to be an electrolyte (a good conductor) in a leathery bag (a poor conductor, an insulator). However, the resistance of the skin is very variable (Table 23.1).
Table 23.1 Electrical resistance of skin
| SKIN TYPE | ELECTRICAL RESISTANCE kΩ cm−2 |
|---|---|
| Mucous membranes | 0.1 |
| Vascular areas (volar aspect of arm, inner thigh) | 0.3–10 |
| Wet skin: in the bath | 1.2–1.5 |
| Sweat | 2.5 |
| Dry skin | 10.0–40 |
| Sole of the foot | 100–200 |
| Heavily calloused palm | 1000–2000 |
Other tissues have diverse electrical resistances, which can be grouped as follows:
There is, however, an idiosyncratic relationship between whole body electrical impedance (AC resistance) and the applied voltage. At low voltages, 25–100 volts, it depends on the state of the skin and area of contact. At 250 volts and higher, the total body impedance falls to 2000–5000 ohm, irrespective of the contact area and the current pathway.3
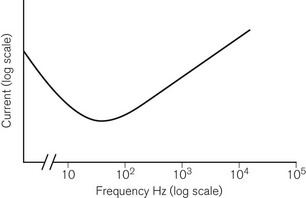
The effects of electric current upon excitable tissues such as muscle and nerve depend not only on current and time, but also on the frequency.4,5 It is one of the ironies of life that the commonly used mains frequencies of 50 Hz (UK, Europe) or 60 Hz (USA) are the frequencies at which the excitable tissues are at greatest risk of excitation and damage (Fig. 23.3).
In greatest danger is the heart, as it is susceptible to induced arrhythmias as well as permanent damage. The direction of the current pathway through the heart is also important. Clinical studies suggest that sudden death from ventricular fibrillation is more likely with current passing ‘horizontally’ from hand to hand, whereas heart muscle damage is more often associated with a ‘vertical’ current pathway.6
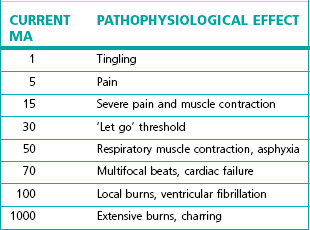
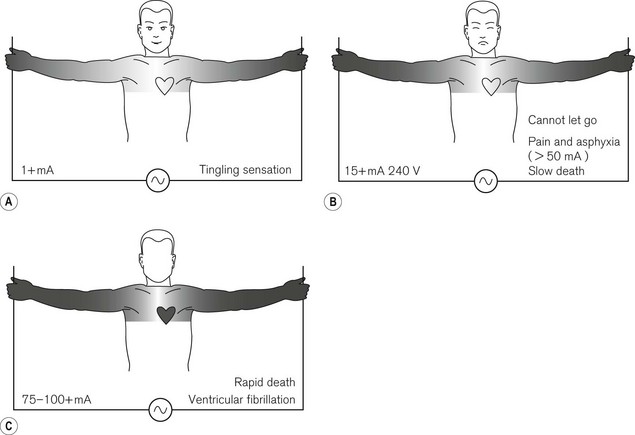
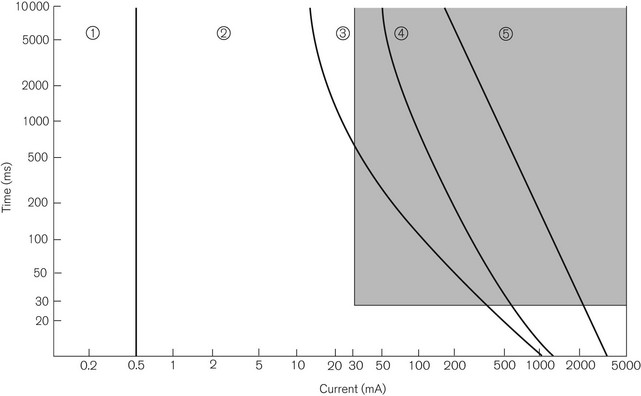
The effects of hand-to-hand 50 Hz AC on the body are shown in Table 23.2 and Fig. 23.4. Fig. 23.5 shows a plot of current magnitude against duration in relation to pathophysiological effects.
Direct current (DC) electric shock tends to result in:
Even very low imperceptible DC may produce electrochemical burns if the current is allowed to pass for long enough, for example from swallowed button-sized 1.5 V hearing aid type batteries.7
Alternating current (AC) electric shock:
• is about three times more dangerous than DC, at similar current flows
• produces continuous muscle contractions (tetany) at 40–110 Hz
• induces grip and pull as flexor muscles are much stronger than extensor muscles. If a person were to be holding onto a faulty conductor, he would be unable to let go. This prolongs the duration of the effect of the current









