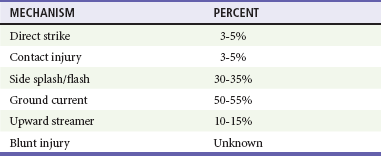
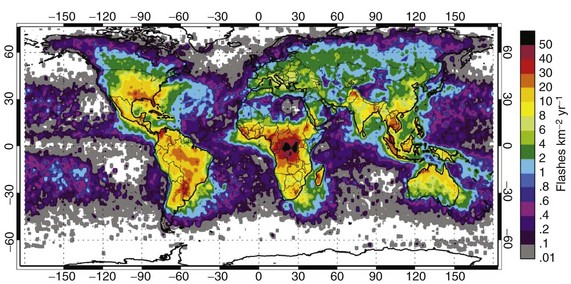
Chapter 142 The first recorded death caused by electrical current from an artificial source was reported in 1879 when a carpenter in Lyons, France, inadvertently contacted a 250-V alternating-current generator.1 The first U.S. fatality occurred in 1881 when an inebriated man passed out on a similar generator in front of a crowd in Buffalo, New York. In the United States, electrical burns account for 4 to 6.5% of all admissions to burn units and approximately 1000 fatalities per year.2 Occupational electrical incidents are uncommon but account for nearly 6% of all occupational fatalities annually.3 Children have a predisposition to injuries from low-voltage sources, such as electric cords, because of their limited mobility within a relatively confined environment. During adolescence, a more active exploration of the environment leads to more severe high-voltage injuries or death. At the time of presentation, documentation of injuries is important not only for the immediate resuscitation of the victim but also for medicolegal reasons. Many electrical injuries eventually involve litigation for negligence, product liability, or worker’s compensation. The incidence of injury and death from lightning is unknown because no agency requires the reporting of lightning injuries, and some victims do not seek treatment at the time of their injury. The incidence of lightning-related deaths in the United States has declined to an average of 39 people annually.4 Lightning is fatal in 1 of 10 lightning strike victims. In typical years, lightning kills more people in the United States than any storm phenomenon except floods, and it is consistently among the top four storm-related killers (Fig. 142-1). In 2009-2010, most of those killed in the United States were within 50 to 100 feet of safety, either seeking safe shelter too late or returning to their outdoor activities before the end of the storm.4 In developing countries, particularly those in the tropics, lightning is a much bigger risk both because it is more common and because agricultural, mining, and construction continue to be labor-intensive, resulting in high exposure to the workers.5 The lack of safe housing and metal vehicles expose entire families and schools to injury whenever a thunderstorm occurs.6 The exact pathophysiologic mechanism of electrical injury is not well understood because of the numerous variables that cannot be measured or controlled when an electrical current passes through tissue. With high voltage, most of the injury is thermal, and histologic studies reveal coagulation necrosis consistent with thermal injury.7,8 The theory of electroporation is that electrical charges insufficient to produce thermal damage cause protein configuration changes that threaten cell wall integrity and cellular function.9 The nature and severity of electrical burn injury are directly proportional to the current strength, resistance, and duration of current flow (Box 142-1).10 Factors that may determine the severity of an electrical injury are summarized in Box 142-2. Unfortunately, none of these can be used to predict or to explain the damage that any individual may suffer. Resistance is the tendency of a material to resist the flow of electrical current. It varies for a given tissue, depending on its moisture content, temperature, and other physical properties. The higher the resistance of a tissue to the flow of current, the greater the potential for transformation of electrical energy to thermal energy. Nerves, designed to carry electrical signals, and muscle and blood vessels, because of their high electrolyte and water content, have a low resistance and are good conductors. Bone, tendon, and fat, which all contain a large amount of inert matrix, have a high resistance and tend to heat and coagulate rather than to transmit current. The other tissues of the body are intermediate in resistance (Box 142-3).11 Skin is the primary resistor to the flow of current into the body. Skin on the inside of the arm or back of the hand has a resistance of approximately 30,000 Ω/cm2. Thick, hardened skin can have 20 to 70 times greater resistance (Table 142-1).8 This high resistance may result in a significant amount of energy being expended at the skin surface as the current burns its way through deep callus, resulting in greater thermal injury to the skin. As the duration of contact increases, however, the skin begins to blister and offer decreased resistance. A surge of current internally can cause extensive deep tissue destruction. Moisture also lowers resistance. Sweating can decrease the skin’s resistance to 2500 to 3000 Ω/cm2, and immersion in water causes a further reduction to 1200 to 1500 Ω/cm2. Table 142-1 The physical effects vary with different amperages at 50 to 60 Hz, which is the AC frequency used in European countries and the United States (Table 142-2). A narrow range exists between the threshold of perception of current (0.2-0.4 mA) and let-go current (6-9 mA). Thoracic tetany can occur at levels just above the let-go current and result in respiratory arrest. Ventricular fibrillation may occur at an amperage of 60 to 120 mA. Although the 120-V household source usually causes minimal injury across dry skin, amperage delivered to the heart when the resistance of the skin is decreased by sweat or submersion in water can result in current sufficient to cause electrocution with cardiac arrest but without apparent external injury. Table 142-2 Physical Effects of Different Amperage Levels at 50 to 60 Hz Current density is the amount of current flow per area of tissue.10 As current density increases, any tendency to flow through the less resistant tissues is overcome. Eventually it flows through tissues indiscriminately, as if the body were a volume conductor, with the potential to destroy all tissues in the current’s path. Because the current is often concentrated at the source and ground contact points, current density and the degree of damage are greatest there. Nevertheless, extensive deep destruction of the tissues may exist between these sites with high-voltage injuries, and the surface damage is often only “the tip of the iceberg.” Damage to the internal structures of the body may be noncontiguous, with areas of normal-appearing tissue adjacent to burned tissue and with damage to structures at sites distant from the apparent contact points. The pathway between contact points is a major determinant of the electrical field strength, which is the voltage per unit of length over which it is applied. For a given current, the shorter the distance between contact points, the greater the electrical field strength. Current from a 20,000-V power line passing from head to toe (approximately 2 m) results in an electrical field strength of 10,000 V/m. Approximately the same electrical field strength is created when “low”-voltage 120-V household current passes between two close contact points on the mouth of a child chewing on a power cord (120 V/0.01 m). Although the electrical field strengths are similar, there is a tremendous difference in the amount of at-risk tissue in the respective pathways.12,13 Although lightning is governed by the same physical laws as artificial electricity is, the rapid rise and decay of the energy complicate predictions of the extent of lightning injury more than with artificial electrical injury. The most important difference between lightning and high-voltage electrical injuries is the duration of exposure to the energy.14 Lightning is neither a direct current nor an alternating current but rather a unidirectional massive current impulse. The cloud-to-ground lightning impulse results from the breakdown of a large electrical field between a cloud and the ground that is measured in millions of volts. When connection is made with the ground, this voltage difference between the cloud and ground disappears, and a large current flows impulsively for a brief instant.14 Mathematical modeling of a lightning flow on the human body, substantiated in animal models, has included only direct strikes that account for only 3 to 5% of lightning injury to people.15,16 After a direct strike meets the body, current is transmitted internally for less than a millisecond before external “flashover” occurs.17 Although lightning current may flow internally for an instant and disrupt electrical systems, it seldom results in significant thermal injury or tissue destruction, and less than one third of lightning survivors have any signs of burns or skin damage. Muscle damage and myoglobinuria from lightning are rare. It is unknown whether the most serious manifestations of lightning injury, cardiac and respiratory arrest, vascular spasm, neurologic damage, and autonomic instability, result from induced electrical changes, current through highly conductive tissues, concussive injury, or other mechanisms. Lightning tends to cause asystole rather than ventricular fibrillation. Although cardiac automaticity may reestablish a rhythm, the duration of the respiratory arrest may cause secondary deterioration of the rhythm to refractory ventricular fibrillation and asystole.14,18 Other injuries caused by blunt trauma or ischemia from vascular spasms, such as myocardial infarction and spinal artery syndromes, also occur.19–22 The primary electrical injury is the burn. Secondary blunt trauma results from falls or being thrown from the electrical source by an intense muscle contraction or the explosive force that may occur with electric flashes from circuit box or transformer accidents. Electrical burns are classified into four different types (Box 142-4). The most destructive indirect injury occurs when a victim becomes part of an electrical arc. An electrical arc is a current spark formed between two objects of differing potential that are not in contact with each other, usually a highly charged source and a ground. The temperature of an electrical arc is approximately 2500° C, and the electrical arc causes deep thermal burns at the point where it contacts the skin.12 With electrical arcs, burns may be caused by the heat of the arc, electrothermal heating due to current flow, or flames that result from the ignition of clothing. Burns may occur from radiated thermal injury when an electrical explosion occurs, similar to gas explosions. Instead of becoming part of the arc, current may appear to jump the gap by splashing across a large part of the body. These splash burns are generally only partial thickness because the person did not become part of the arc itself.23 At the time of presentation it is often difficult to determine the mechanism of injury that caused an electrically injured patient’s burns. Electrothermal heating is the main cause of muscle damage and is seen almost exclusively in high-voltage accidents with prolonged (seconds) contact and current flow.23 The histologic change in muscle injury that results from direct contact with an electrical source is coagulation necrosis with shortening of the sarcomere.8,11 Muscle damage can be erratic, so areas of viable and nonviable muscle are often found in the same muscle group. Periosteal muscle damage may occur even though overlying muscle appears to be normal. Similar to muscle damage, serious vascular damage usually occurs only after a high-voltage accident. Vascular damage is greatest in the media, predisposing to delayed hemorrhage when the vessel eventually ruptures.11 Intimal damage may result in either immediate or delayed thrombosis and vascular occlusion as edema and clots form on the damaged intimal surface of the vessel during a period of days. The injury is usually most severe in the small muscle branches, where blood flow is slower.24 This damage to small muscle arteries combined with mixed muscle viability that is not visible to gross inspection creates the illusion of progressive tissue necrosis. Veins, having more sluggish flow, are more prone to thrombosis than arteries are, and significant distal edema can result. The hands, feet, and skull are the most common contact points. Histologic studies of the brain reveal focal petechial hemorrhages in the brainstem, cerebral edema, and widespread chromatolysis (the disintegration of chromophil bodies of neurons).11 Lightning injury may occur by electrical mechanisms and by secondary concussive or blunt trauma.16,25 Whereas direct strike is most commonly described as the mechanism of injury, studies show that it accounts for a very small proportion of injuries and deaths (Table 142-3). Table 142-3 Distribution of Lightning Injury Mechanisms From Cooper MA, Holle RL: Mechanisms of lightning injury should affect lightning safety messages. Presented at the 3rd International Lightning Meteorology Conference, Orlando, Fla, April 2010. Injury from contact occurs when the person is touching an object that is part of the pathway of lightning current, such as a tree, metal fence, indoor plumbing, or wiring. Side flash or splash occurs as a portion of lightning jumps from its primary strike object to a nearby person on its way to the ground.11,14,16,19,26 Step voltage, a difference in electrical potential between a person’s feet, may occur as lightning current spreads radially through the ground.14,16 A person who has one foot closer than the other to the strike point has a potential difference between the feet so that a portion of the lightning current flows through the legs and body rather than the ground. This ground current is a common killer of large livestock such as cattle and horses because of the greater distance between their hind legs and forelegs, with the heart lying in the pathway. People may also be injured by upward streamers.25 Cloud-to-ground lightning approaches the earth as a downward stepped leader. As the leader approaches, the large electrical field induces opposite charges that surge through trees, buildings, people, and any other object near the thunderstorm. If one of these upward streamers connects with a downward leader, a completed lightning strike occurs. Individuals in the path of an upward streamer may be injured even in the absence of a completed lightning strike. Ball lightning is a mobile, luminous, spheroidal, floating or bouncing ball that lasts a few seconds before suddenly vanishing or exploding. These glowing orbs are observed traveling down power lines and aisles of aircraft and even entering buildings through open doors.27 Although ball lightning has been described by multiple reputable observers for many years, the origin, chemical makeup, and physics are still a mystery. Blunt injury from lightning can occur from at least two mechanisms. First, the person may be thrown a considerable distance by the sudden, massive contraction caused by current passing through the body. Second, a concussive injury caused by explosive or implosive force occurs as the lightning pathway is instantaneously superheated then rapidly cooled after the passage of the lightning.14 This concussive injury or barotrauma is associated with tympanic membrane rupture, contusions of various organs, and pneumothorax.28–33 Blunt or concussive injury can also accompany electrical injury.
Electrical and Lightning Injuries
Perspective
Lightning Injury
Principles of Disease
Resistance
TISSUE
RESISTANCE (Ω/cm2)
Mucous membranes
100
Vascular areas
Volar arm, inner thigh
300-10,000
Wet skin
Bathtub
1200-1500
Sweat
2500
Other skin
10,000-40,000
Sole of foot
100,000-200,000
Heavily calloused palm
1-2 million
Amperage
PHYSICAL EFFECT
CURRENT (mA)
Tingling sensation
1-4
Let-go current
Children
4
Women
7
Men
9
Freezing to circuit
10-20
Respiratory arrest from thoracic muscle tetany
20-50
Ventricular fibrillation
60-120
Pathway
Mechanisms of Injury
Lightning Injury

Full access? Get Clinical Tree


Electrical and Lightning Injuries


Only gold members can continue reading. Log In or Register to continue





{kind=link}