Fig. 67.1
Mitral valve systole

Fig. 67.2
Mitral valve diastole
I. A 70-year-old male with long-standing history of a cardiac murmur presents for evaluation of decreased exertion tolerance. He has no other significant past medical or surgical history. He previously was very active and walked 2–3 miles daily but recently has had to cut back to one mile due to fatigue and dyspnea. Physical exam is notable for a 3/6 holosystolic murmur located at the apex and radiating to the axilla, a laterally displaced apical impulse and an early diastolic rumble. A transthoracic echocardiogram (TTE) is obtained which prompts a transesophageal echocardiogram (TEE) for further evaluation.
Questions
- 1.
What is the normal anatomy of the mitral valve?
- 2.
- 3.
How is mitral regurgitation classified?
- 4.
What is the role of 3D TEE in the evaluation of mitral regurgitation?
- 5.
What are the advantages and disadvantages of three-dimensional (3D) echocardiography compared to two-dimensional (2D) echocardiography?
- 6.
What are the indications for surgical treatment of mitral regurgitation?
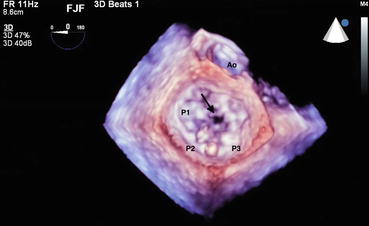
Fig. 67.3
Mitral valve systole
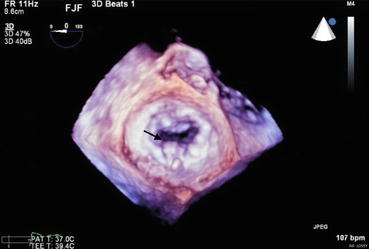
Fig. 67.4
Mitral valve diastole
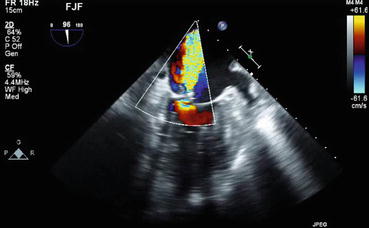
Fig. 67.5
Mitral regurgitation
II. A 40 year old female with hypertension, diabetes, and end-stage renal disease on hemodialysis presents to the emergency room complaining of a 2 week history of fevers, chills, night sweats and a 1 day history of rapidly progressive shortness of breath. She is sitting upright, in moderate distress and appears dyspneic. Temperature is 38.4°C. 2/2 blood cultures grow S. aureus. Physical exam reveals an S3 and an early diastolic flow rumble.
Answers
- 1.
The mitral valve is the left atrioventricular (AV) valve. It is a bileaflet valve composed of anterior (aortic) and posterior (mural) leaflets. The anterior mitral valve leaflet (AML) occupies 1/3 of the mitral annulus but is broader and occupies 2/3 of the surface area of the valve. It is in fibrous continuity with the left and non-coronary cusps of the aortic valve. The posterior mitral valve leaflet (PML) occupies 2/3 of the mitral annulus but only accounts for 1/3 of the surface area of the valve [1]. It is divided into three scallops which Carpentier labeled P1, P2 and P3 going laterally to medially. By convention, the AML is similarly divided into three segments (A1, A2, A3 from lateral to medial) which correspond to the PML scallops. The mitral annulus is fibrous anteriorly, muscular posteriorly, and changes shape during the cardiac cycle. The muscular posterior portion is more prone to dilatation and calcification. On the ventricular aspect of the mitral valve, there are three layers of chordae tendinae (primary, secondary and tertiary) which attach to the papillary muscles. There are classically two papillary muscles: posteromedial and anterolateral. The posteromedial papillary muscle is connected via cords to the medial 1/2 of the mitral valve and the anterolateral papillary muscle gives cords to the lateral 1/2 of the mitral valve. With normal mitral valve function, there is a zone of coaptation where the leaflets close, as well as a 4–5 mm zone of apposition where the two leaflets overlap.
- 2.
Figures 70.1 and 70.2 show the classical 3D TEE surgeon’s view of the mitral valve in systole (Fig. 67.1) and diastole (Fig. 67.2). In the surgeon’s view, the left atrium has been opened and you are looking down at an en face view of the mitral valve. The aortic valve by convention is at the top of the image. In this view, the lateral commissure and left atrial appendage are to the left of the image, and the medial commissure and tricuspid valve apparatus are to the right of the image. PML scallops are labeled by the Carpentier convention, lateral to medial, P1, P2 and P3. The adjacent segments of the AML are labeled A1, A2, A3 from lateral to medial. These images show a flail P2 segment due to a ruptured cord (arrow). A flail segment is defined as the tip of the leaflet pointing towards the left atrium in systole and the left ventricle in diastole.Related posts:

Full access? Get Clinical Tree




