Ear, Nose, and Throat
5-1 Sinusitis
Matthew Spencer
Clinical Presentation
Acute sinusitis consists of persistent purulent nasal discharge, cough, unilateral facial pain and fullness, fever, nasal congestion, maxillary or periorbital swelling, and headache.1 Patients who are ill-appearing, with a fever of at least 39°C and purulent nasal discharge for 3 to 4 days, are considered to be more severely affected.1 On physical examination, there is often sinus tenderness and opacification of the affected sinus with transillumination, but these findings are considered unreliable.2
Pathophysiology
Sinusitis is a bacterial infection of the paranasal sinuses. Sinusitis is classified as acute, subacute, or chronic, based on the duration of symptoms. Sinusitis is acute if the infection has been present for less than 4 weeks.1,3 In subacute sinusitis, symptoms have been present for 1 to 3 months. Sinusitis is considered to be chronic if symptoms have been present for longer than 3 months.1 Sinusitis develops when there is inflammation of the paranasal sinus mucosa, usually secondary to allergies or viral infection. Inflammation leads to mucosal edema, excessive mucus production, decreased fluid clearance, and then bacterial overgrowth.1,2,4 Bacterial overgrowth usually consists of the normal respiratory flora, with Streptococcus pneumoniae present in 30% to 66% of cases, Haemophilus influenzae in 20% to 30%, Moraxella catarrhalis in 12% to 30%, and Streptococcus pyogenes in 3% to 7%.1,2,4 Fungal organisms occasionally are the etiologic cause of acute sinusitis in diabetics and patients with other types of immunocompromise.2,4
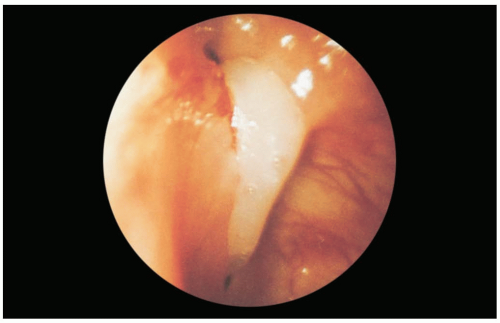 FIGURE 5-1 Accessory maxillary sinus ostium with purulent drainage. (From Benjamin, with permission.) |
Diagnosis
Acute sinusitis usually is a clinical diagnosis. However, the gold standard requires needle aspiration of the maxillary sinus, although this procedure is not usually performed in the emergency department.1
Various clinical criteria may differentiate bacterial from viral sinusitis. Some consider purulent nasal discharge and cough that persists for 10 to 14 days, with a history of preceding upper respiratory tract infection, to be diagnostic.1 Others use a combination of major and minor clinical criteria. Major criteria are facial pain or pressure, facial fullness, nasal obstruction, purulent nasal discharge, decreased sense of smell, and fever.2 Minor criteria are headache, halitosis, fatigue, dental pain, cough, ear pain, ear pressure, and ear fullness.2 The presence of any two major criteria or one major plus two minor criteria is considered diagnostic.2 Another group found four clinical criteria that correlated significantly with computed tomography (CT)-confirmed sinusitis: acute worsening of symptoms after some improvement, a history of purulent nasal secretions, purulent nasal secretions present on examination, and an elevated erythrocyte sedimentation rate (ESR).2,3,4 None of these methods is perfect, but the diagnosis is highly likely if symptoms have persisted for longer than 10 days with an acute worsening at some time during this period, if purulent nasal secretions are present, if there has been no response to decongestants, or if fever or other severe symptoms are present.4
Plain radiographs are not considered to be of value in most patients with possible sinusitis, and CT has been shown to overdiagnose the disease.4 However, despite the risk of overdiagnosis, CT is the radiographic modality of choice; it should be used primarily for patients in whom the diagnosis is uncertain, for those with suspected orbital or intracranial complications, for those with no response to adequate therapy, and to define anatomy in preparation for surgery.1,2,4
Clinical Complications
Management
Treatment consists of antibiotics, decongestants, and symptomatic therapies. First-line antibiotics should be inexpensive, with high-dose amoxicillin the drug of choice and trimethoprim-sulfamethoxazole, azithromycin, and clarithromycin possible agents for penicillin-allergic patients.1,2,4 Common second-line agents are amoxicillin/clavulanate, cefpodoxime, cefuroxime, cefdinir, cefprozil, and the fluoroquinolones.1,2,4 All antibiotics should be continued for 10 to 14 days.1 Patients with complications, frequent recurrences, or treatment failures should be referred to an ear, nose, and throat (ENT) specialist.2,4
REFERENCES
1. Conrad DA, Jenson HB. Management of acute bacterial rhinosinusitis. Curr Opin Pediatr 2002;14:86-90.
2. Brook I, Gooch WM 3rd, Jenkins SG, et al. Medical management of acute bacterial sinusitis: recommendations of a clinical advisory committee on pediatric and adult sinusitis. Ann Otol Rhinol Laryngol Suppl 2000;182:2-20.
3. Lindbaek M, Hjortdahl P. The clinical diagnosis of acute purulent sinusitis in general practice: a review. Br J Gen Pract 2002;52:491-495.
4. Poole MD. A focus on acute sinusitis in adults: changes in disease management. Am J Med 1999;106:38S-47S.
5-2 Allergic Rhinitis
Andrew Gorlin
Clinical Presentation
In the acute phase (within 5 minutes after exposure to the allergen), allergic rhinitis manifests as sneezing, nasal itching, and watery rhinorrhea. During the late phase (4 to 8 hours after exposure), the main symptom of allergic rhinitis is nasal congestion.1,2 Chronic allergic rhinitis results in postnasal drip with chronic cough, headache, nasal voice, and systemic symptoms such as malaise, irritability, and decreased appetite.2 On physical examination, a boggy, pale-blue nasal mucosa, clear secretions, and swollen turbinates are found. More subtle symptoms include the “allergic salute,” in which the patient repetitively rubs his nose upward with his palm, and the resultant “allergic crease,” a transverse skin line below the bridge of the nose.1
Pathophysiology
Seasonal allergic rhinitis is caused by airborne allergens released by seasonal vegetation such as ragweed, grass, and tree pollen. Perennial allergic rhinitis results from exposure to allergens such as animal dander, molds, and dust. Regardless of the type of allergen, the precipitating event is immunoglobulin E binding of the allergen, with subsequent mast cell and basophil activation. Activated mast cells and basophils in the nasal mucosa release histamine, leukotrienes, prostaglandins, and other inflammatory mediators that cause local edema, increased mucus secretion, and cellular infiltration.2
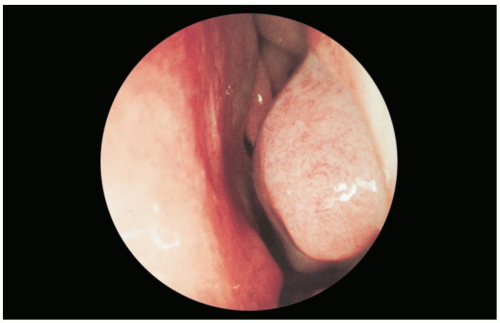 FIGURE 5-2 This swollen, bluish, left inferior turbinate is pathognomonic for allergic rhinitis. (From Benjamin, with permission.) |
Diagnosis
The history and physical examination are key to the diagnosis of allergic rhinitis. Eosinophilia identified on a nasal smear can aid diagnosis; a positive smear is defined as greater than 10% eosinophils (normal, 2% to 3%). Definitive diagnosis requires skin testing.1
Clinical Complications
Common sequelae include otitis media (OM) and sinusitis secondary to obstruction of the eustachian tube and sinus ostia, respectively. Other sequelae include decreased olfaction and taste, snoring, sleep apnea, and, in developing children, facial abnormalities such as high-arched palate and dental malocclusion due to chronic mouth breathing.
Management
Allergic rhinitis is managed in the outpatient setting. Removal of the inciting allergen and use of allergenproof products in the home is an important first step in treatment. Oral antihistamines, topical corticosteroids, and oral and topical α-adrenergic agents are the mainstays of pharmacologic therapy. Severe refractory cases may be treated with immunotherapy.1,2
REFERENCES
1. McNamara RM. Approach to rhinitis. Emerg Med Clin North Am 1987;5:279-292.
2. Berger WE. Overview of allergic rhinitis. Ann Allergy Asthma Immunol 2003;90[6 Suppl 3]:7-12.
5-3 Viral Rhinitis
Andrew Gorlin
Clinical Presentation
Patients with viral rhinitis, also known as the “common cold,” present with rhinorrhea, sneezing, nasal congestion, sore throat, and low-grade fever.
Pathophysiology
Human rhinovirus causes more than 50% of cases of viral rhinitis, followed by coronavirus (20%), influenza, adenovirus, and respiratory syncytial virus.1,2,3 Infection starts with local invasion of the epithelial surface of the nasal mucosa. Viral replication ensues, with cell death and subsequent viral spread. Infection triggers the cellular release of cytokines and chemotactic factors, resulting in local edema, mucus secretion, and influx of neutrophils and lymphocytes.2,3
Diagnosis
The history and physical examination usually are sufficient to diagnose viral rhinitis. Diagnostic testing is rarely indicated. A nasal smear may distinguish viral rhinitis from allergic rhinitis by the lack of eosinophilia. Viral culture can provide a definitive diagnosis.1 Physical examination findings include a red, edematous nasal mucosa, with nasal secretions varying from watery and clear to thick and mucoid. Patients also may have injected conjunctivae and oropharynx, as well as sinus tenderness. The condition is self-limited, with symptoms usually peaking 2 to 4 days after viral inoculation.1
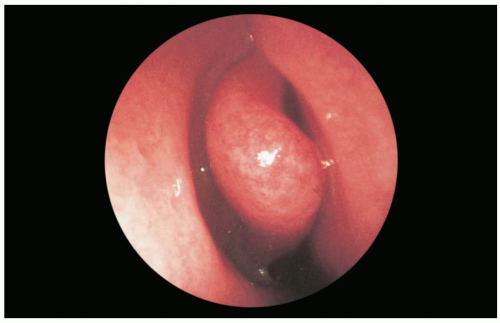 FIGURE 5-3 During the prodromal phase of acute viral rhinitis, the mucous membranes lining the nasal cavity are reddened, the nose is often abnormally patent, and the patient usually complains of an itching or burning inside the nose. (From Benjamin, with permission.) |
Clinical Complications
The most frequent complication of viral rhinitis is bacterial sinusitis, which occurs secondary to inflammatory obstruction of the sinus ostia. Bacterial superinfection of the nasal mucosa may also occur. Streptococcal species are noted to be the predominate bacteria in these conditions.1
Management
Most cases of viral rhinitis are mild and self-limited and can be managed in the outpatient setting. Hand washing and basic hygiene are sensible preventative measures. Oral and topical α-adrenergic agents are the most commonly used agents for symptomatic relief. Topical steroids are also effective, but they are not universally recommended because of potential immunosuppression. There is no role for antihistamines in viral rhinitis. Antibiotics are indicated only for secondary bacterial infections.1,2
REFERENCES
1. McNamara RM. Approach to rhinitis. Emerg Med Clin North Am 1987;5:279-292.
2. Winther B, Gwaltney JM Jr, Mygind N, Hendley JO. Viral-induced rhinitis. Am J Rhinol 1998;12:17-20.
3. van Cauwenberge P, Ingels K. Effects of viral and bacterial infection on nasal and sinus mucosa. Acta Otolaryngol 1996;116:316-321.
5-4 Anterior Epistaxis
Matthew Spencer
Clinical Presentation
Patients with anterior epistaxis (AE) present with bleeding from one or both nostrils. AE is more common in younger patients but can be seen in all age groups. The bleeding is usually less profuse than in posterior epistaxis, and a source is often visible on the nasal septum.
Pathophysiology
AE originates from Kiesselbach’s plexus, an area of convergence of multiple blood vessels located on the anterior of the nasal septum.1,2 Bleeding has been associated with various causes, including low humidity, trauma, inflammation, allergies, hypertension, coagulation abnormalities, and anticoagulant or antiplatelet medications.2 Most adult cases are idiopathic, whereas those in children usually are caused by digital trauma.2,3
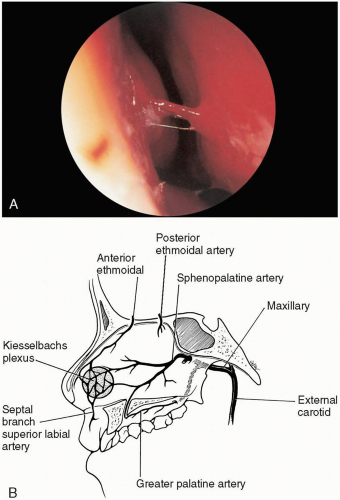 FIGURE 5-4 A: Anterior-nasal-septum with active bleeding. (From Benjamin, with permission.) B: Note location of Kiesselbach’s plexus, the most common site of anterior bleeding. (From Cotton, with permission.) |
Diagnosis
The diagnosis of AE is clinical. However, it is difficult to distinguish posterior epistaxis from AE; severity of bleeding, lack of response to initial treatment modalities, and quantity of blood in the oropharynx should be considered.3
Clinical Complications
Management
Initial treatment includes digital pressure to the nose.2,3 If direct pressure succeeds but a point source is not identified, the patient is observed for 60 minutes for rebleeding and discharged with instructions to use saline nasal spray three times per day and to apply a petroleum-based antibiotic ointment daily. A point source of bleeding should be identified for cautery, if possible.1
If bleeding persists, the nose should be packed. Use of packing soaked with agents such as oxymetazoline 0.5%, phenylephrine HC1 1%, pseudoephedrine, or epinephrine (1:10,000), plus either lidocaine 2% to 4% or Pontocaine (tetracaine), is approriate.1,2 Cocaine 4% may be used, because it is both an anesthetic and a vasoconstrictor.1,2,3 If an anterior source is identified after the nasal mucosa is anesthetized, it should be cauterized with silver nitrate.1,2,3 One should never cauterize both sides of the nasal septum, because this may lead to a perforation.
If anterior nasal packing successfully stops the bleeding, it should be left in place for 2 to 3 days, the patient should be prescribed oral antibiotics to cover staphylococcal and streptococcal species, and follow-up should be arranged within 1 to 3 days.1,2 If anterior nasal packing is unsuccessful, then a posterior source should be suspected.
REFERENCES
1. Tan LK, Calhoun KH. Epistaxis. Med Clin North Am 1999;83:43-56.
2. Pashen D, Stevens M. Management of epistaxis in general practice. Aust Fam Physician 2002;31:717-721.
3. Chopra R. Epistaxis: a review. J R Soc Health 2000;120:31-33.
5-5 Posterior Epistaxis
Matthew Spencer
Clinical Presentation
Patients with posterior epistaxis present with profuse bleeding from one or both nostrils, with the large amount of swallowed blood and blood visible in oropharynx.1,2,3 In one study, 88% of clinicians reported the bleeding as moderate or severe.3 Occasionally, brisk anterior nosebleeds produce similar findings.
Pathophysiology
Posterior epistaxis is bleeding that originates from the posterior nasopharynx, usually the sphenopalatine artery or Woodruff’s plexus. Epistaxis may result from damage to the nasal epithelium caused by a variety of factors, including low humidity, trauma, inflammation, allergies, hypertension, bleeding abnormalities, and anticoagulant or antiplatelet medications.2,3,4
 FIGURE 5-5 Active bleeding from the posterior septum is visible in the posterior pharynx. (Courtesy of Mark Silverberg, MD.) |
Diagnosis
The diagnosis is clinical. However, it is difficult to distinguish posterior epistaxis from AE; the severity of bleeding, lack of response to initial treatment modalities, and quantity of blood in the oropharynx must all be taken into consideration.3
Clinical Complications
Management
Initial treatment includes digital pressure, cotton or tissue packing, having the patient lean forward so that the blood runs out of the mouth instead of down the throat, and cold compresses to the bridge of the nose.2,5 If a posterior source is suspected, posterior nasal packing must be performed as quickly as possible. One method is to insert a Foley catheter through the nostril into the oropharynx, inflate the balloon, and then withdraw the catheter to exert pressure from the balloon against the choana.1 Other catheters are available for this purpose, such as balloon catheters made by Brighton and Simpson (West Sussex, U.K.) that are specifically designed for posterior nasal packing.2,4 These patients should all be admitted to the intensive care unit (ICU) for sedation, intravenous fluid therapy, and oxygen administration, because the complications from posterior nasal packing are severe. The packing material must be left in place for 48 to 72 hours.3 Emergency, on-site consultation with an otolaryngologist must be obtained in all cases of posterior bleeding.1,2,4
REFERENCES
1. Sparacino LL. Epistaxis management: what’s new and what’s noteworthy. Lippincott’s Prim Care Pract 2000;4:498-507.
2. Tan LK, Calhoun KH. Epistaxis. Med Clin North Am 1999;83:43-56.
3. Viducich RA, Blanda MP, Gerson LW. Posterior epistaxis: clinical features and acute complications. Ann Emerg Med 1995;25:592-596.
4. Chopra R. Epistaxis: a review. J R Soc Health 2000;120:31-33.
5-6 Zygomatic Arch Fracture
Matthew Spencer
Clinical Presentation
Patients with zygomatic arch fracture present with a history of facial trauma, trismus, facial ecchymosis, and edema. In many cases, facial asymmetry due to flattening of the malar eminence and tenderness over the zygoma are clearly present.1,2 Isolated arch fractures often produce only severe swelling and pain; without radiographic studies, the condition may not be apparent for up to 1 week, after local swelling has diminished.1 If there is associated diplopia, enophthalmos, ptosis, or infraorbital nerve hypoesthesia or anesthesia, a zygomaticomaxillary (ZMC) fracture should be suspected.1,3
Pathophysiology
Zygomatic arch fractures result from trauma, most commonly secondary to motor vehicle collisions, assaults, or athletics.2 Zygomatic fractures are the third most common facial fractures.2 ZMC fractures, which are more common than isolated arch fractures, involve the body of the zygoma, orbital floor, and maxillary sinus wall.1,2
Diagnosis
The diagnosis should be suspected if a patient presents with a history of facial trauma and a characteristic clinical examination. However, the diagnosis must be confirmed radiographically. A Waters view and a submentovertex (SMV) view usually are adequate to diagnose an isolated zygomatic arch fracture, but if more extensive fractures are suspected, axial and coronal computed tomography (CT) with 2- to 3-mm cuts is necessary.1,2
Clinical Complications
Management
The treatment in the emergency department consists of analgesics, ice packs to reduce swelling, and prompt consultation with an otolaryngologist or plastic or oral surgeon, because these fractures usually are repaired by open reduction and internal fixation.2,3 Fracture reduction does not have to be immediate; it may be delayed 4 to 7 days to allow the edema to subside.2
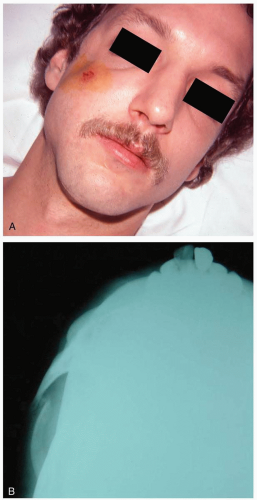 FIGURE 5-6 A: Facial depression indicative of zygomatic arch fracture. (Courtesy of Michael Greenberg, MD.) B: X-ray film showing “jug-handle” view of zygomatic arch. (Courtesy of Mark Silverberg, MD.) |
REFERENCES
1. Ellis E III, Scott K. Assessment of patients with facial fractures. Emerg Med Clin North Am 2000;18:411-448.
2. Carithers JS, Koch BB. Evaluation and management of facial fractures. Am Fam Physician 1997;55:2675-2682.
3. Greenberg AM. Management of facial fractures. N Y State Dent J 1998;64:42-47.
4. Zingg M, Laedrach K, Chen J, et al. Classification and treatment of zygomatic fractures: a review of 1,025 cases. J Oral Maxillofac Surg 1992;50:778-790.
5-7 Orbital Floor Fracture
Matthew Spencer
Clinical Presentation
Patients with orbital floor fracture present after facial trauma with periorbital edema and ecchymosis associated with tenderness to palpation along the inferior orbital rim.2,3,4 Subconjunctival hemorrhage, enophthalmos, or a palpable step-off of the orbital rim may also be present.1,2,3,4 Diplopia may be present, or the patient may experience limited globe mobility if entrapment of one or more of the extraocular muscles also exists.3
Pathophysiology
Orbital floor fractures are more common in adults and are seen in 10% of head injuries.1,2,3 The classic “blowout fracture” is hypothesized to result from a hard object striking the orbit anteriorly and pushing its contents backward, leading to increased intraorbital pressure and a break in the weakest portion of the bony orbit, the medial floor.3,4
Diagnosis
The diagnosis should be suspected in the setting of trauma with periorbital edema and tenderness, and it is more likely if entrapment is clinically evident. The Waters view of facial plain films often reveals such a fracture or shows a “teardrop sign.” The diagnostic modality of choice is the orbital computed tomography (CT).1,2,3,4
Clinical Complications
Complications include infraorbital anesthesia, ptosis or pseudoptosis, diplopia, lacrimal duct injury, medial and lateral canthus injuries, and corneal abrasions or lacerations. More severe injuries associated with orbital floor fractures are hyphema, retinal hemorrhages, retrobulbar and vitreous hemorrhages, globe displacement or injury, glaucoma, and blindness.1,3
Management
The mainstay of therapy in the emergency department is analgesics, ice to reduce swelling, and consultation with an ophthalmologist; ear, nose, and throat (ENT); or plastic surgery specialist. Treatment in both adults and children is controversial and varies depending on the consultant. Antibiotic therapy is controversial with these injuries and should be considered in the consultations.4
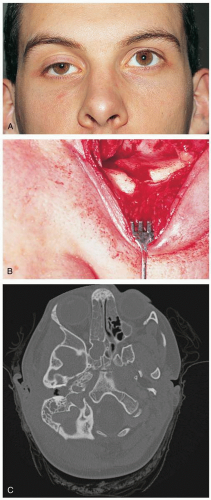 FIGURE 5-7 A: Pseudoptosis: enophthalmos secondary to an orbital blowout fracture. (From Tasman, with permission.) B: A direct fracture of the orbital floor extends from the infraorbital rim. (From Tasman, with permission.) C: Computed tomogram showing right orbital fracture. (Courtesy of Robert Hendrickson, MD.) |
REFERENCES
1. McDonald WS, Thaller SR. Priorities in the treatment of facial fractures for the millennium. J Craniofac Surg 2000;11:97-105.
2. Koltai PJ, Rabkin D. Management of facial trauma in children. Pediatr Clin North Am 1996;43:1253-1275.
3. Roncevic R, Roncevic D. Extensive, traumatic fractures of the orbit in war and peace time. J Craniofac Surg 1999;10:284-300.
4. Carithers JS, Koch BB. Evaluation and management of facial fractures. Am Fam Physician 1997;55:2675-2682.
5-8 Nasal Septal Hematoma
Matthew Spencer
Clinical Presentation
Patients with nasal septal hematoma typically present to the emergency department complaining of nasal pain after facial trauma. They may occasionally report unilateral nasal obstruction.1 On physical examination, the hematoma appears as a purple swelling of the nasal mucosa that arises from the septum, bulges into the nostril, and may cause either partial or complete obstruction.1,2 The hematoma usually feels soft when palpated with a cotton swab or finger and should not change size with topical vasoconstrictors.1,2
 FIGURE 5-8 Large right-sided septal hematoma causing septal deviation to the left. (© Philip Mead, MD. Used with permission.) |
Pathophysiology
A nasal septal hematoma results from accumulation of blood between the perichondrium and the cartilage of the nasal septum after nasal trauma.2 Nasal septal hematomas accumulate after injury to the internal lining of the septal perichondrium, resulting in blood accumulation between the perichondrium and the cartilage.1,2
Diagnosis
The diagnosis usually is made based on clinical findings in the setting of trauma. A nasal speculum may be necessary to properly visualize the nasal septum.1
Clinical Complications
Complications of a septal hematoma are often severe and include abscess formation (most common), aseptic septal necrosis, intracranial infection, and septum perforation with saddle deformity.1
Management
REFERENCES
1. Koltai PJ, Rabkin D. Management of facial trauma in children. Pediatr Clin North Am 1996;43:1253-1275.
2. Ginsburg CM. Nasal septal hematoma. Pediatr Rev 1998;19:142-143.
5-9 Parotitis
Matthew Spencer
Clinical Presentation
Patients with parotitis present with fever and unilateral erythema, swelling, and warmth lateral to the angle of the mandible.1
Pathophysiology
Acute suppurative parotitis results from bacterial infection of the parotid gland.1 Risk factors for infection include dehydration, recent surgery or anesthesia, advanced age, prematurity, radiation therapy, immune compromise, sialolithiasis, and oral neoplasm.1 The most common bacterial cause is Staphylococcus aureus, but S. pyogenes and α-hemolytic Streptococcus species are also encountered.1 The most common viral causes are mumps and paramyxovirus, but other species have been implicated.1
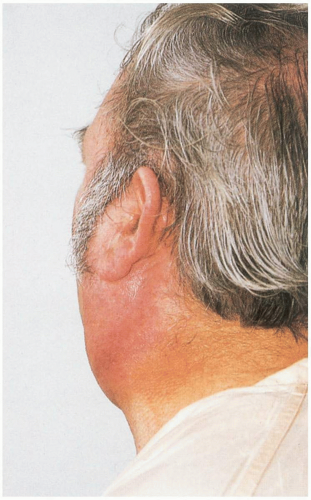 FIGURE 5-9 Left-sided parotid abscess with swelling and redness. (From Benjamin, with permission.) |
Diagnosis
The diagnosis of suppurative parotitis can be made clinically with the expression of pus from Stensen’s duct or by needle aspiration.1 The diagnosis of viral parotitis may be assumed if the patient exhibits the classic prodromal history in conjunction with localized parotid inflammation. Viral parotitis usually manifests after a 1- to 5-day prodrome of low-grade fever, headache, myalgias, and malaise.1 The gland then becomes swollen and painful, and ear pain, trismus, and dysphagia may also develop. Pus should not be expressible from the duct (in contrast to bacterial parotitis).1 Viral parotitis is bilateral 75% of the time.1
Clinical Complications
Complications include septicemia, mandibular osteomyelitis, fascial extension, airway obstruction, mediastinitis, internal jugular vein thrombosis, and facial nerve dysfunction.1 Mumps has been reported to lead to meningoencephalitis, pancreatitis, orchitis, myocarditis, pericarditis, arthritis, and nephritis.1
Management
Patients with parotitis should be treated with warm compresses, sialagogues such as lemon drops, and external parotid massage.1 Intravenous fluids may be necessary to prevent dehydration due to limited oral intake. Broad-spectrum oral antibiotics covering Staphylococcus and Streptococcus species should be initiated if bacterial infection is suspected and the patient is stable and nontoxic in appearance.1 First-line agents include dicloxacillin and cephalexin.1 If the response is suboptimal or the patient is ill and dehydrated, intravenous antibiotics may be more appropriate.1 Ampicillin-sulbactam, oxacillin, methicillin, and the second-generation cephalosporins are adequate single agents.1 Incision and drainage should be considered if an abscess is present, if there is facial nerve involvement, or if there is lateral neck extension. The treatment for viral parotitis is supportive.1
REFERENCES
1. McQuone SJ. Acute viral and bacterial infections of the salivary glands. Otolaryngol Clin North Am 1999;32:793-811.
5-10 Temporomandibular Joint Syndrome
Matthew Spencer
Clinical Presentation
Patients with temporomandibular joint (TMJ) syndrome complain of unilateral (90%), deep, dull, aching pain that may become sharp and radiate across the face or temple.1 On physical examination, there may be trismus, TMJ “clicking,” limitation of jaw movement, deviation of the jaw to the side with opening, and tenderness at the insertion of the lateral pterygoid muscle.1,2
Pathophysiology
TMJ syndrome is thought to be caused by spasm of the pterygoid muscles.1 Risk factors include a history of bruxism, trauma, recent dental work, anxiety, cradling of the telephone between the jaw and shoulder, and malocclusion.1
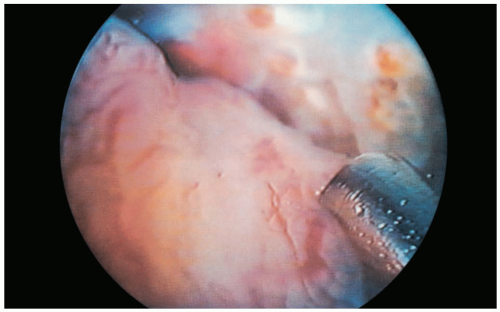 FIGURE 5-10 Synovitis of the temporomandibular joint may be treated with laser synovectomy, as shown here. (From Benjamin, with permission.) |
Diagnosis
The diagnosis is made from the history and physical examination. Radiographs are rarely helpful except in cases of suspected arthropathy.1
Management
Treatment is multifactorial and includes stress reduction, decrease in intake of caffeine and nicotine, muscle massage, jaw muscle exercises, and regular aerobic exercise.2 In the emergency department, patients should be treated with analgesics and muscle relaxants, with recommendations for several days of soft diet, heat to the affected areas, and referral to an oral surgeon or otolaryngologist within 1 to 2 weeks.2
REFERENCES
1. Jones NS. Classification and diagnosis of facial pain. Hosp Med 2001;62:598-606.
2. Blank LW. Clinical guidelines for managing mandibular dysfunction. Gen Dent 1998;46:592-597.
5-11 Acute Mastoiditis
Matthew Spencer
Clinical Presentation
Before antibiotic therapy for acute otitis media (OM) became widely available, mastoiditis was the most common complication of OM (up to 20% of patients).1,2,3 In the postantibiotic era, mastoiditis has become uncommon, with an incidence of only 0.2% to 2%.2 It primarily affects young children, with the peak age at onset being 6 to 36 months. Patients usually present with pain and tenderness of the postauricular area, followed by swelling and erythema. The pinna of the ear is often displaced forward, and the tympanic membrane (TM) is usually thickened, inflamed, dull, and immobile.1,2,3
Pathophysiology
Mastoiditis results from a middle ear infection that causes mucosal swelling and blockage of the passage between the middle ear and the mastoid air cells (the aditus ad antrum).1,2 This inflammation leads to impaired mastoid drainage, fluid accumulation in the air cells that provides a hospitable environment for bacterial growth, and eventually infection.1,2 There appears to be a spectrum of disease. In the first stage, known as acute mastoiditis with periostitis, the infection is confined to the periosteum and mucosa of the mastoid air cells. The second stage, acute coalescent mastoiditis, occurs when the infection extends beyond the periosteum and bony destruction of the air cells develops.1 The most common cause is S. pneumoniae, followed by H. influenzae and S. pyogenes.1,2 Other, less commonly implicated organisms include Proteus mirabilis, Streptococcus hominis, M. catarrhalis, and S. aureus.2,3
 FIGURE 5-11 Swelling, redness, and adenopathy in the area of the left mastoid. (Courtesy of Mark Silverberg, MD.) |
Diagnosis
The diagnosis is a clinical one, with confirmation by radiographic imaging studies. Plain radiographs of the mastoid region generally are not useful.2 Computed tomography (CT) is the preferred means for determining the presence or absence of fluid or pus collections in the mastoid cells.
Clinical Complications
Management
REFERENCES
1. Fliss DM, Leiberman A, Dagan R. Acute and chronic mastoiditis in children. Adv Pediatr Infect Dis 1997;13:165-185.
2. Spratley J, Silveira H, Alvarez I, Pais-Clemente M. Acute mastoiditis in children: review of current status. Int J Pediatr Otorhinolaryngol 2000;56:33-40.
3. Wang NE, Burg JM. Mastoiditis: a case-based review. Pediatr Emerg Care 1998;14:290-292.
5-12 Perichondritis
Matthew Spencer
Clinical Presentation
Patients with perichondritis present with pain, redness, swelling, warmth, and tenderness of the involved ear.1,2 Often the ear lobe, which does not contain cartilage, is not involved; this finding can be helpful in distinguishing perichondritis from cellulitis.2
 FIGURE 5-12 Acute perichondritis secondary to pinna trauma. (From Benjamin, with permission.) |
Pathophysiology
Diagnosis
The diagnosis is made by history and physical examination; no radiographic studies are necessary.
Clinical Complications
Management
REFERENCES
1. Templer J, Renner GJ. Injuries of the external ear. Otolaryngol Clin North Am 1990;23:1003-1018.
2. Yahalom S, Eliashar R. Perichondritis: a complication of piercing auricular cartilage. Postgrad Med J 2003;79:29.
3. Bassiouny A. Perichondritis of the auricle. Laryngoscope 1981;91:422-431.
5-13 Cauliflower Ear
Matthew Spencer
Clinical Presentation
Pathophysiology
The term cauliflower ear is used to describe a deformity of the external ear that results from an improperly or incompletely treated perichondral hematoma.1,2,3 This injury is commonly seen in wrestlers and boxers at the high school and college level, who may sustain repeated trauma to the ear.3 CE develops secondary to hematoma formation between the perichondrium and the underlying cartilage. As the locally accumulated blood clot resolves, the perichondrium is stimulated to produce new cartilage in an irregular pattern as it heals.1,2 These deformities are more commonly associated with blunt and tractional trauma, but they can develop after penetrating injuries (as a result of persistent subcutaneous bleeding after laceration repair).2
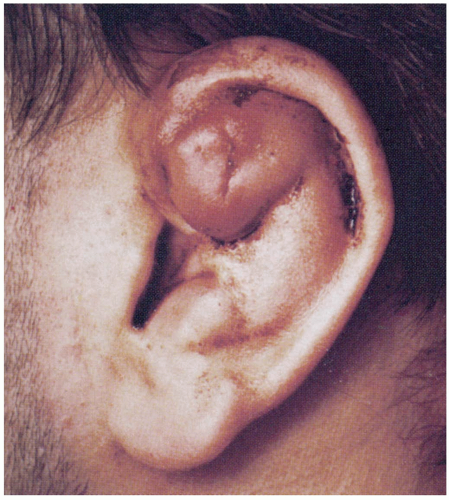 FIGURE 5-13 Cauliflower ear. (From Khalak R. Images in clinical medicine: cauliflower ear. N Engl J Med 1996;335:399.) |
Diagnosis
The diagnosis of CE is made clinically. The ear is usually tender to palpation and may be ecchymotic. If the ear injury is old, CE may be an incidental finding on physical examination. The diagnosis of CE is based on a history of ear trauma in conjunction with the development of a characteristic deformity, ranging from a mild cartilaginous thickening to severe irregular deformity of the pinna. This may eventually result in the development of a fleshy growth of the ear that resembles a piece of cauliflower.
Clinical Complications
Management
To prevent the development of a CE, the initial perichondral hematoma must be drained and a pressure dressing applied to prevent its reaccumulation.1 Drainage of the hematoma may be performed by either incision and drainage or needle aspiration performed under local anesthesia.1,2,3 If the hematoma needs to be aspirated on more than one occasion, it should be incised and drained.2 Oral antibiotics are not routinely necessary. However, antibiotic coverage is clearly indicated in the immunocompromised patient.1
REFERENCES
1. Lee D, Sperling N. Initial management of auricular trauma. Am Fam Physician 1996;53:2339-2344.
2. Chudnofsky CR, Sebastian S. Special wounds: nail bed, planter puncture, and cartilage. Emerg Med Clin North Am 1992;10:801-822.
3. Templer J, Renner GJ. Injuries of the external ear. Otolaryngol Clin North Am 1990;23:1003-1018.
5-14 Otitis Externa
Matthew Spencer
Clinical Presentation
Patients with otitis externa (OE) present with otalgia, otorrhea, pruritus, redness, and swelling of the auditory canal.
Pathophysiology
OE consists of three clinical stages.1 The preinflammatory stage develops when the lipid layer of the external auditory canal is removed by moisture or trauma, leading to swelling that causes obstruction, ear fullness, and pruritus.1 The inflammatory stage ranges from mild to severe and progresses from only slight edema, erythema, and clear discharge to total canal obstruction with large amounts of purulent discharge and debris.1 The chronic stage consists of low-grade inflammation and infection that persists despite therapy.1 Causes for OE range from bacterial and fungal infection to eczema. The most common causative bacteria are S. aureus, P. aeruginosa, Proteus vulgaris, and streptococci. Fungal infections are common in diabetics, and Aspergillus and Candida are the common causative strains.1,2,3,4 Risk factors for OE include persistent moisture, local irritants, systemic diseases, and local trauma.1,4
Diagnosis
OE is a clinical diagnosis. Swab cultures may provide diagnostic confirmation but are not useful in acute treatment.
Clinical Complications
Complications include chondritis, parotitis, ear canal stenosis, chronic otitis, hearing deficits, and malignant OE.
Management
Treatment consists of local cleaning and debris removal, topical medication, oral analgesics, and education on methods of prevention. Various ear drops are available, including 2% acetic acid preparations, polymyxin B/neomycin/hydrocortisone, ciprofloxacin/hydrocortisone, and ofloxicin.1,2,3,4 Quinolone or aminoglycoside ophthalmic solutions should be used if other otic preparations are not tolerated, because they are less acidic and less irritating. Ear drops should be administered as 3 to 4 drops four times per day for 3 days beyond the resolution of symptoms, or for a total of 7 to 10 days, whichever is longer. More severe infections may require 10 to 14 days of therapy.1 Ear drops should be placed directly into the ear canal, or on a cotton wick inserted into the canal if there is severe swelling of the canal. Fungal OE requires treatment with clotrimazole, tolnaftate, or natamycin.1,2,3 Oral analgesics such as acetaminophen, ibuprofen, or acetaminophen/narcotic combinations are commonly required. Referral to an otolaryngologist should be considered for recurrent or resistant cases.4
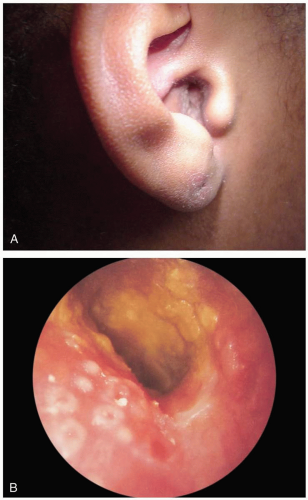 FIGURE 5-14 Otitis externa. A: View of infected ear. (Courtesy of Christy Salvaggio, MD.) B: View of macerated external canal. (From Benjamin, with permission.) |
REFERENCES
1. Hughes E, Lee JH. Otitis externa. Pediatr Rev 2001;22:191-197.
2. Biedlingmaier JF. Two ear problems you may not need to refer: otitis externa and bullous myringitis. Postgrad Med 1994;96:141-145,148.
3. Schapowal A. Otitis externa: a clinical overview. Ear Nose Throat J 2002;81[8 Suppl 1]:21-22.
4. Sander R. Otitis externa: a practical guide to treatment and prevention. Am Fam Physician 2001;63:927-936,941-942.
5-15 Malignant Otitis Externa
Matthew Spencer
Clinical Presentation
Most patients with malignant otitis externa (MOE) present with acute onset of severe otalgia (often worse at night), otorrhea, a feeling of ear fullness, and loss of hearing.1
Pathophysiology
MOE, also called necrotizing otitis externa (OE), is a severe infection of the external auditory canal that usually is caused by infection with P. aeruginosa.1,2 It is often a disease of elderly diabetic patients, with an average age of 65 years. However, it has also been described in middle-aged and pediatric patients with immune system compromise.1,2,3 Bacterial invasion occurs through clefts in the cartilage of the external auditory canal, leading to infection of the soft tissues at the base of the skull.3
Diagnosis
The diagnosis usually is clinical and should be suspected if there is no improvement or a worsening of symptoms in a patient with adequately treated OE, or if the pain is out of proportion to the findings on clinical examination. The external auditory canal usually is swollen and erythematous, with a purulent discharge, and the pinna of the ear often is inflamed and tender.3 Granulation tissue may be present at the bony cartilaginous junction of the ear. Fever and lymphadenopathy are not common, and the white blood cell count usually is normal. computed tomography (CT), magnetic resonance imaging (MRI), and radionuclide imaging are useful in confirming the diagnosis and delineating the extent of infection.1,3 Radionuclide imaging and the erythrocyte sedimentation rate (ESR) are also frequently used to monitor the response to therapy.
Related posts:







Full access? Get Clinical Tree


