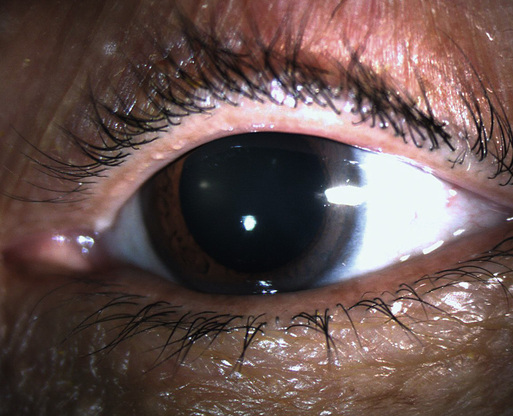
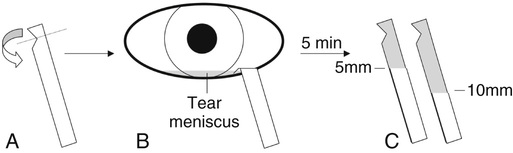
Scott D. Walter, James T. Banta Dry eye is a multifactorial disorder characterized by abnormalities in the tear film that result in symptoms of discomfort, visual disturbance, and tear film instability with potential damage to the ocular surface.1 The disorder is known by many names including dry eye syndrome, ocular surface disease, keratoconjunctivitis sicca, aqueous tear film deficiency, and dysfunctional tear syndrome. Dry eye is one of the most common reasons that adults consult an eye care professional. It is also treated frequently by primary care physicians, and, perhaps most commonly, by patients themselves. Prevalence estimates for dry eye have varied widely, ranging from as low as 0.6% to as high as 57% based on the population studied and the stringency of the definition of the disease.2 Several large cross-sectional studies have estimated that 5 million Americans have moderate to severe dry eye disease, and up to 20% of the population report occasional dry eye symptoms.3 Dry eye is a surprisingly complex condition. The tear film is responsible for nourishing and lubricating the ocular surface, as well as providing its immune protection. In addition, the tear film functions as the anterior refracting surface of the eye and, as such, plays a pivotal role in maintaining optical clarity. A healthy tear film is created by complex interactions of the lacrimal glands and ducts, cornea and conjunctiva, eyelids, and meibomian glands and is maintained by autonomic and reflexive functions of the peripheral somatosensory and motor nervous system.1 The tear film itself is formed with each blink and is composed of three layers: an inner mucin layer, an intermediate aqueous layer, and an outer lipid layer. The outer lipid layer, produced largely by secretions of the meibomian glands in the upper and lower eyelids, limits evaporative loss of the underlying aqueous layer between blinks. A deficiency in any layer of the tear film or in any component of the lacrimal functional unit can lead to dry eye. Broadly speaking, dry eye can be classified into two mechanistic categories: aqueous-deficient and evaporative dry eye. Aqueous-deficient dry eye typically localizes to the lacrimal gland, and lacrimal gland insufficiency may be caused by Sjögren disease (a primary or secondary autoimmune infiltration of the lacrimal and salivary glands leading to dry eye and dry mouth), other infiltrative diseases of the lacrimal gland, or primary hyposecretion. Evaporative dry eye similarly has many causes, although the most common is meibomian gland dysfunction, in which the lipid-producing meibomian glands in the eyelids are obstructed at their openings (Fig. 75-1). Other causes of evaporative dry eye include poor eyelid closure (lagophthalmos), inadequate blinking, and ocular rosacea. Despite the apparent simplicity of this classification scheme, most patients with dry eye will have components of both mechanisms contributing to their disease. Regardless of the cause, inflammation plays a central role in exacerbating and perpetuating dry eye disease. Inflammatory cytokines affect tear film osmolarity, leading to increased tear film instability and evaporative loss, which in turn leads to further inflammation.4 Breaking this inflammatory cycle is critical in the management of dry eye disease.5 As the disease becomes more chronic, dry eye may evolve into a corneal pain disorder. There is increasing evidence that a significant number of patients with chronic dry eye describe features of neuropathic pain.6 Dysfunctional adaptation of the corneal pain apparatus, including changes in corneal nerve morphology and neurotransmission,7,8 may also contribute to the development of a more persistently symptomatic disease phenotype.9 The symptoms of dry eye may be vague and nonspecific, and the clinician must carefully distinguish dry eye from other conditions that affect the ocular surface. Patients with dry eye most often have a chief concern of dryness, foreign body sensation (a scratchy or gritty feeling in the eyes), burning or stinging pain, itching, or ocular fatigue. They may also secondarily complain of redness or light sensitivity or note transient blurred vision that is relieved by blinking. Often their symptoms are worsened by activities that require visual concentration (e.g., reading or computer use) or by low-humidity environments (e.g., airplane travel). Paradoxically, some patients may demonstrate excessive tearing, a reflexive hypersecretion of tears caused by corneal irritation. Many contact lens users report increasing intolerance to their lenses. A careful medical history, including current medications and a complete review of systems, should be obtained, because many systemic diseases and treatments can cause or exacerbate the symptoms of dry eyes. For example, many commonly prescribed anticholinergic drugs (including antihistamines and tricyclic antidepressants), alpha blockers (e.g., tamsulosin), antihypertensives (including diuretics and beta blockers), oral corticosteroids, and even vitamins have been associated with dry eye symptoms.10 Autoimmune diseases including lupus and rheumatoid arthritis can cause a secondary Sjögren syndrome leading to aqueous-deficient dry eye. Similarly, infiltrative processes affecting the lacrimal gland, such as lymphoma, sarcoidosis, and graft-versus-host disease, can cause lacrimal gland insufficiency. Thyrotoxicosis and thyroid eye disease can cause exophthalmos, eyelid retraction, and incomplete eyelid closure.11 Cranial nerve VII (e.g., Bell) palsies causing partial or complete paralysis of the orbicularis oculi muscle may also lead to eyelid malposition, poor eyelid closure, and exposure of the ocular surface. Reactivation of varicella zoster virus (shingles) within the ophthalmic division of the trigeminal nerve may lead to diminished corneal sensation, an impaired blink reflex, and exposure of the ocular surface.12 Decreased corneal sensitivity and lower rates of spontaneous blinking are also seen in patients with Parkinson disease.13 Physical examination by the primary care physician should include measurement of visual acuity (in each eye separately) as well as an external inspection of the ocular adnexa, including the skin, eyelids, conjunctiva, and cornea. If available, fluorescein dye can be used in conjunction with a cobalt blue–filtered light source to highlight pathology on the corneal surface. Attention should be given to eyelid and cranial nerve (especially V and VII) function, because incomplete eyelid closure (lagophthalmos) can cause corneal exposure and evaporative dry eye. The primary care physician should evaluate for eyelid retraction and proptosis (hallmarks of thyroid eye disease) and consider screening for thyroid dysfunction. In addition, a complete physical examination—with close attention to the skin and joints—should be completed to screen for an associated autoimmune condition. Although examination of the ocular surface by an ophthalmologist can help establish a diagnosis of dry eye syndrome, there is often a poor correlation between signs and symptoms in dry eye syndrome.16 Some patients will report severe symptoms with little objective evidence of ocular surface disease; others will note only mild symptoms despite dramatic findings clinically. This discrepancy between signs and symptoms can complicate the diagnosis and management of patients with dry eye. The diagnosis of dry eye is based primarily on symptoms subjectively reported by the patient. The Ocular Surface Disease Index (OSDI) is a simple, reliable, and reproducible way to assess dry eye severity and to monitor patients’ response to treatment.14 Two basic tests help to distinguish aqueous-deficient from evaporative dry eye. • A Schirmer test can be performed to assess aqueous production (Fig. 75-2). A narrow piece of filter paper is placed in the inferior cul-de-sac, and tear production is measured by the amount the paper is wet after 5 minutes. The test can be performed with topical anesthesia (to measure basal tearing) or without anesthesia (to measure basal plus reflex tearing). A cutoff of less than 5 mm (with anesthesia) or less than 10 mm (without anesthesia) is considered abnormal.15 An abnormal Schirmer test result suggests aqueous-deficient dry eye. • For patients with aqueous-deficient dry eye suspected of having Sjögren syndrome, a serologic evaluation including SS-A (anti-Ro), SS-B (anti-La), rheumatoid factor, and antinuclear antibodies should be obtained.15
Dry Eye Syndrome
Definition and Epidemiology
Pathophysiology
Clinical Presentation
Physical Examination
Diagnostics
Related posts:

Full access? Get Clinical Tree


Dry Eye Syndrome
Chapter 75