Emergency Treatment of Disorders Due to Cold
Individuals vary considerably in their response to environmental cold. Factors that increase the possibility of injury due to cold include poor general physical condition, nonacclimatization, childhood or advanced age, systemic illness, and the use of alcohol and other sedative drugs. High wind velocity (wind-chill factor) and moisture may markedly increase the propensity for cold injury at low temperatures.
- Signs and symptoms depend on degree of hypothermia
- Rewarming methods include passive external, active external, and active internal rewarming
Accidental hypothermia occurs when an external cold challenge overwhelms an individual’s capacity to produce or conserve heat. Hypothermia may occur in otherwise healthy individuals during occupational or recreational exposure to cold or as a result of accidents or other misfortunes. Alcohol and drug abuse is a common predisposing cause.
Systemic hypothermia may follow exposure to even slightly lowered temperatures when preexisting altered homeostasis exists as a result of debility or disease. Accidental hypothermia is more likely to occur in elderly or inactive people and those with cardiovascular, dermatologic, or cerebrovascular disease; mental retardation; myxedema; hypopituitarism; or alcoholism. The use of sedative–hypnotic or antidepressant drugs may be a contributing factor.
Because lowered body temperature is the sole finding in some patients brought to the emergency department, the diagnosis often depends on awareness of the possibility of hypothermia.
In the hypothermic patient, oral and axillary temperatures are not accurate. Instead, rectal probes should be used. The temperature varies widely in hypothermia, and accurate monitoring is essential.
Hypothermia is classified as mild when core body temperature is between 34°C (93.2°F) and 36°C (96.8°F). Patients will exhibit tachycardia, tachypnea, and shivering. Hypothermia is moderate between 30°C (86°F) and 34°C. Loss of the shivering reflex and mild alterations in level of consciousness occur. Bradycardia and atrial fibrillation may start to appear. Hypothermia becomes severe below temperatures of 30°C. Patients may appear dead at this stage with fixed, dilated pupils, loss of other reflexes, and coma.
Ventricular fibrillation and asystole may occur spontaneously at core temperatures below 28°C (82.4°F). Note: For this reason, a hypothermic patient should not be considered dead until all reasonable resuscitative measures have failed. No one is dead until he or she is “warm and dead.”
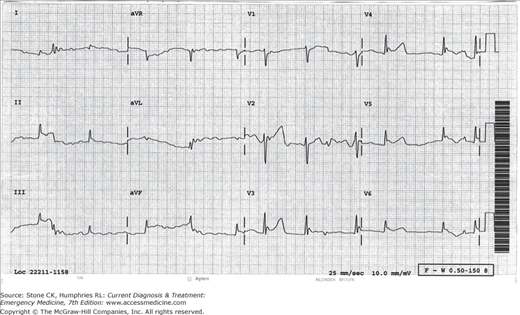
Several laboratory findings are unique to hypothermia. Hypoglycemia, hypomagnesemia, and hypophosphatemia are common, particularly in alcoholics. Hyperglycemia may be seen as a result of hemorrhagic pancreatitis in patients with prolonged exposure to the cold. Sodium and potassium levels may be elevated or depressed. Arterial blood gas samples drawn at cold temperatures are generally analyzed at 37°C (98.6°F), which causes lowering of pH and elevation of PO2 and PCO2 readings. However, clinical therapy is based on the uncorrected determinations recorded at 37°C.The ECG tracing may show prolongation of any conduction interval. Osborne or J wave, may appear below 32°C (89.6°F) (Figure 46–1).
Metabolic acidosis, pneumonia, pancreatitis, renal failure, sepsis, and ventricular fibrillation may occur. Death due to systemic hypothermia usually results from cardiac arrest associated with ventricular fibrillation, which may occur during rewarming.
Obtain a brief history from witnesses or relatives of a patient with hypothermia, and perform a general physical and laboratory examination to detect underlying conditions that might predispose to hypothermia.
Examination should include an evaluation of renal function (uremia), thyroid function (myxedema), and adrenal function (Addison disease). If sepsis is a diagnostic possibility, obtain appropriate cultures.
Bundle the victim of suspected hypothermia in dry, warm blankets at the scene of discovery, and transport the person to the nearest hospital as soon as possible. Remove any wet garments. Note: Transport should be as gentle as possible because of the risk of cardiac arrhythmias due to increased myocardial irritability.
Adequacy of ventilation and circulation must be ensured by careful clinical observation, continuous ECG monitoring, and serial determinations of arterial blood gases. If cardiac arrest occurs, start cardiopulmonary resuscitation (CPR) (Chapter 9). If the victim has any detectable pulse or breathing, no matter how slow, do not initiate CPR; unnecessary brisk closed chest compression may induce ventricular fibrillation. Because of the protective effects of hypothermia, bradycardia and hypotension are generally well tolerated.
Intubation of the unprotected airway and frequent suctioning may be required.
Depression of the respiratory center in hypothermia causes hypoxemia or hypercapnia, requiring controlled ventilation and supplemental oxygen. Avoid hyperventilation, because a rapid fall in Pco2 may trigger ventricular fibrillation.
Check for a pulse for at least 1 minute. If a pulse is present, do not attempt to correct arrhythmia with drugs or cardioversion. This will be unsuccessful most of the time and may precipitate ventricular fibrillation. Begin the rewarming process (see below). If the patient is pulseless, begin CPR. Attempts at defibrillation are usually unsuccessful at temperatures below 30°C (86°F). If ventricular tachycardia/fibrillation is present, attempt a shock at 360 J. If there is no success, continue CPR. At temperatures less than 30°C, withhold further defibrillation and intravenous medications. Begin aggressive rewarming in conjunction with basic CPR. If temperature is 30°C or greater, then continue with ACLS protocol but space intravenous medications longer than standard (decreased metabolism may induce toxicity of drugs).
Give thiamine (100 mg intravenously), naloxone (2.0 mg intravenously), and dextrose (25 g intravenously) to all patients with altered mental status who are thought to be hypothermic. Volume expansion with warmed fluid generally helps the rewarming process. Avoid lactated Ringer’s solution because the lactate is not metabolized efficiently by a cold liver.
Treat underlying and predisposing conditions as necessary (eg, heart disease, hypoglycemia, malnutrition, adrenocortical insufficiency [hydrocortisone, 200 mg intravenously], hypothyroidism [levothyroxine, 400 micrograms intravenously, plus hydrocortisone, 100 mg intravenously]).
Rewarming is essential but potentially harmful, because peripheral vasodilatation may divert blood flow from internal organs to the skin and shunt cooled blood to the central circulation, causing a brief drop in core temperature. Note: Rapid rewarming may be hazardous, because hypothermic patients are particularly vulnerable to lethal cardiac arrhythmias. Core rewarming should be undertaken only if hypothermia is severe and the patient shows cardiovascular instability (eg, cardiac arrest and ventricular fibrillation).
Passive rewarming to prevent further heat loss is sufficient for most patients with mild hypothermia, because their thermoregulatory mechanism is intact, and many of these patients are able to generate heat by shivering. Most patients should be wrapped in dry, heated blankets and carefully monitored. Ambient air temperature can be warmed with radiant heat sources. Patients with mild hypothermia who are otherwise healthy usually respond well to heated blankets and the administration of heated (45°C [113°F]) intravenous solutions. Patients must be carefully monitored when using any of these rewarming methods.
Moderate to severe hypothermia often requires additional rewarming measures, because thermoregulation is altered or absent. Individualized supportive care is mandatory, because active rewarming is hazardous. As mentioned previously, active core rewarming is necessary only for patients with cardiovascular instability.
Heated blankets, forced-air blankets (Bair Hugger), or warm baths have been used, with a rate of rewarming of about 1–3°C/h. Because it is easier to monitor the patient and to carry out diagnostic and therapeutic procedures when heated blankets rather than warm baths are used for active rewarming, heated baths are not widely recommended. There is some potential risk with active external rewarming, because marked vasodilation may occur. Combining active external rewarming with active core rewarming may prevent the resultant hypotension and the core temperature after-drop, which are sometimes seen during rewarming. If active external rewarming is used, the patient should be carefully monitored and supported hemodynamically. The application of commercial heat packs directly to hypothermic skin may cause serious burns.
Internal rewarming is suggested for patients with profound hypothermia of long duration in which there is suspected underlying debilitation, for patients with complications of cardiovascular or respiratory insufficiency, and for patients in cardiac arrest.
Repeated peritoneal dialysis may be performed using warm (45°C [113°F]) potassium-free dialysate solution or normal saline. The usual exchange rate is 6 L/h, which can increase the core temperature 1–3°C/h.
Warm fluids (crystalloid solutions) administered by gastrointestinal, colonic, or bladder lavage may be employed. Placement of a nasogastric tube is less invasive but may run the risk of stimulating ventricular dysrhythmias owing to the irritability of the hypothermic heart.
Administration of heated intravenous fluids contributes only 17 kcal/h, which accounts for an increase in body temperature of less than 1/3°C/L. Microwave rewarming of crystalloid solutions to 40–42°C (104–107.6°F) may be safely accomplished in about 2–3 minutes. This technique causes some hemolysis of erythrocytes, and if blood products are used they should be administered through a high-flow countercurrent fluid infuser or reconstituted with warmed normal saline.
Heated humidified oxygen, either via a tight-fitting mask or by endotracheal tube, will raise the core temperature 1 or 1.5–2°C/h, respectively.
Thoracic cavity lavage may achieve rapid rewarming with the added advantage of warming the heart more quickly. Insert two thoracostomy tubes, and continuously infuse fluid warmed to 41°C (105.8°F) through one tube and drain it through the other.
Extracorporeal blood rewarming methods are the gold standard for rewarming in the setting of severe cardiorespiratory compromise/arrest. This may be accomplished via cardiopulmonary bypass or hemodialysis. These methods of course are limited to the institutions that have the abilities to perform these functions.
Patients with severe hypothermia—especially those who are comatose—are at high risk for development of aspiration pneumonia; subsequent pulmonary, urinary tract, or intraperitoneal infections; and sepsis. Many hypothermic alcoholic, debilitated, or elderly patients will have an underlying infection, and the cause should be aggressively sought and treatment initiated.
If sepsis suspected, administer broad-spectrum antibiotics. Prophylactic antimicrobial drugs are unnecessary if infection is unlikely.
Observe the patient for signs of metabolic acidosis, cardiac arrhythmias, acute respiratory distress syndrome, pancreatitis, ischemic bowel, pneumonia, myoglobinuria with renal failure, or clotting abnormalities.
Hospitalize all patients who present with core temperatures below 34°C (93.2°F), especially if the sensorium is altered. Patients with coexisting illness and core temperatures under 35°C (95°F) should be hospitalized. The mortality rates in hypothermia are variable and depend on the cause of hypothermia and the patient’s underlying condition.
- Tissue injury or death is caused by ischemia and thrombosis in capillaries or by formation of ice in the tissues
- Treatment of frostbite or chilblains depends on the severity of the skin injury and includes rewarming by both passive and active measures
In healthy individuals, exposure of the extremities to cold produces immediate localized vasoconstriction followed by reflex generalized vasoconstriction. When skin temperature falls to 25°C (77°F), tissue metabolism is slowed, but the relative demand for oxygen exceeds the supply from diminished circulation; thus, the area becomes cyanotic. At 15°C (59°F), tissue metabolism is markedly decreased and the dissociation of oxyhemoglobin is reduced, which may give the skin a pink, well-oxygenated appearance. Tissue damage occurs at this temperature. Tissue death may be caused either by ischemia and thrombosis in capillaries or by actual freezing. Frostbite is tissue freezing caused by formation of ice crystals in tissue. Frostbite occurs when skin temperature drops to 10–4°C (14–24.8 °F). The body’s “hunting reaction,” serves to protect the extremity from cold injury by alternating vasoconstriction with vasodilation in 5–10 minute cycles. This occurs with exposure to progressively colder temperatures. The incidence of frostbite depends on factors such as wind, moisture, mobility, venous stasis, trauma, malnutrition, and occlusive arterial disease.
Chilblains, occurs with exposure to nonfreezing temperatures and is more common in children and women as well as people with any form of peripheral vascular disease. Chilblains are red or violaceous, painful skin lesions common on the ears, nose, hands, and feet. Lymphocytic vasculitis is common. Chilblains may be associated with edema or blistering and are subsequently aggravated by excessive warmth. With continued exposure, ulcerative or hemorrhagic lesions may appear and progress to scarring, fibrosis, and atrophy.
Treatment of chilblains is mainly supportive. Elevate the affected part on pillows or sheepskin, and allow it to warm gradually at room temperature.
Do not rub or massage injured tissues or apply ice or heat. Protect the area from trauma and secondary infection. Refer the patient to a primary-care physician or clinic for follow-up. Nicardipine and steroids may also have a role in treatment.
Frostbite is injury of the tissues due to freezing. The classification of injury is applied after rewarming, because the extent of injury is difficult to predict initially. Demarcation is not complete for up to 3–5 weeks.
Freezing without blistering; peeling is occasionally present.
Freezing with clear blistering.
Freezing with death of skin, hemorrhagic blisters, and subcutaneous involvement.
Freezing with full-thickness involvement (including bone); ultimate loss or deformity of body part.
Frostbitten tissue appears white or blue–white, is firm or hard (frozen), cool to the touch, and generally insensitive. Skin loses sensation at around 10°C. Because cold injury produces anesthesia, many symptoms are not apparent until rewarming begins or the part is closely inspected. In patients with mild frostbite, the symptoms are numbness, paresthesias, pruritus, and lack of fine motor control. With increasing severity, decreased range of motion, blister formation, and prominent swelling are noted. Thawing unmasks local tenderness and throbbing pain. The tissue becomes discolored, loses its elasticity, and becomes immobile. Profound edema, hemorrhagic blisters, necrosis, and gangrene may occur. Long-term sequel includes cold sensitivity, loss of sensation, and hyperhidrosis.
Treat moderate to severe associated systemic hypothermia before managing frostbite.
Rewarm extremities affected by superficial frostbite (frostnip) by removing wet clothing and applying constant warmth, which can be accomplished by exerting gentle pressure with a warm hand.
Rapid rewarming is the most important aspect of management. It should not be attempted, however, if the potential for refreezing exists. Rewarming should be performed with a water bath or whirlpool containing an antimicrobial agent such as iodine or chlorhexidine. Water temperature of 40–42°C (104–107.6°F) is necessary. However, The State of Alaska Cold-injury Guidelines recommend a lower temperature of 37–39°C (98.6–102.2°F). This temperature causes less pain for the patient and only slightly prolongs rewarming. Rewarming should continue until a red-purple color appears and the skin becomes pliable. Recommended rewarming time is anywhere from 15 inutes up to 1 hour.
Unless concomitant hypothermia exists, intravenous hydration is not usually necessary. Severe cases of frostbite have led to subsequent rhabdomyolysis with renal failure, which then requires aggressive hydration. Intravenous narcotics are almost always necessary secondary to the severe pain associated with rewarming.
In the prehospital setting, padding, splinting, and avoidance of rewarming are all that is necessary. Once in the secure hospital setting and after rewarming has been achieved, avoidance of further trauma is important. Affected body parts should be elevated and padded, uncovered or loosely dressed, and left at room temperature. Debride clear blisters because prostaglandins and thromboxane are present in the exudate. Leave hemorrhagic blisters intact. Administer antitetanus prophylaxis. Apply aloe vera cream every 6 hours. Administer ibuprofen, 400–600 mg every 8–12 hours for 72 hours.
Infection prevention is important after rewarming. Maintain a sterile environment. Protect skin blebs from physical contact. Whirlpool therapy at temperatures of 32–38°C (89.6–100.4°F) twice daily for 30 minutes for a period of 3 or more weeks helps to cleanse the skin and debride superficial dead tissue. Penicillin prophylaxis is recommended in most cases.
Consistent benefit from anticoagulation has not been demonstrated.
Have been used with some success.
Small clinical studies with tissue plasminogen activator have demonstrated success in humans, but the results of larger, multicenter trials are needed.
Amputation or debridement should not be considered until it is definitely established that tissues are dead. Although rare, the development of a compartment syndrome necessitates fasciotomy. The line of demarcation between injured and normal tissue may not appear until 6–12 weeks after injury; mummification of the injured extremity may require the same length of time. Technetium-99 pyrophosphate and MRI scanning accurately predicts the level of ultimate amputation. Regional sympathectomy performed 24–48 hours after injury has reportedly ameliorated the early sequel of frostbite, including a reduction in edema and decreased subsequent tissue loss. Appropriate clinical studies have yet to be performed to support the use of this therapy.
Disagreement still exists as to effectiveness of HBO therapy. Recent studies in humans have yielded good results.
Hospitalize all patients with second- or third-degree frostbite and patients with extensive areas of first-degree frostbite.
- Caused by prolonged immersion in cold water
- Alternating vasospasm and vasodilatation results in initial cold and anesthetic feet followed by blistering and ulceration
- Treatment includes rewarming and wound care
Immersion foot (or hand) is caused by prolonged immersion in cool or cold water or mud that causes alternating arterial vasospasm and vasodilatation. The affected parts are first cold and anesthetic. Hyperemia follows after 24–48 hours, and the parts become warm, with intense burning and tingling pain. Blistering, swelling, redness, ecchymoses, and ulceration are noted. The posthyperemic phase occurs after 2–6 weeks and causes the limbs to become cyanotic, with increased sensitivity to cold. Complications include lymphangitis, cellulitis, thrombophlebitis, and wet gangrene.
Changing out of wet socks and shoes as soon as possible is paramount to the prevention of immersion syndrome. In the military, individuals at risk for immersion foot apply silicone ointment to the bottoms of their feet twice daily as a preventive measure.
Treatment is best started during or before the stage of reactive hyperemia.
Immediate treatment consists of protecting the extremities from trauma and secondary infection. Rewarm the injured areas gradually by exposing them to air (not to ice or extreme heat). Do not soak or massage the skin. The patient should remain at bed rest until all ulcers have healed. Keep the affected parts elevated to aid in removal of edema fluid, and protect pressure sites (eg, heels) with pillows or booties lined with cotton batting. Give antimicrobials only if infection occurs.
Hospitalize all patients with immersion syndrome.
1This chapter is a revision of the chapter by Shannon Waters, MD, from the 5th edition.
Emergency Treatment of Disorders Due to Heat
The five main disorders due to environmental heat stress are (1) heat edema, (2) heat syncope, (3) heat cramps, (4) heat exhaustion, and (5) heat stroke.
The body maintains temperature homeostasis via four main mechanisms: (1) conduction, (2) convection, (3) radiation, and (4) evaporation. When the body is unable to adequately regulate body temperature using these methods, heat illness occurs. The extremely young and old, obese, and those with chronic physical and mental impairments have the highest risk of heat illness. The fully heat acclimatized and athletic, healthy individuals are also at risk, however, given the right environmental conditions, if they are impaired by drugs or alcohol, or if they are denied access to hydration and nutrition.
- Swelling of feet and ankles due to vasodilatation and venous stasis
- Treatment is elevation of the limbs
Nonacclimatized individuals, particularly the elderly, may develop swelling of the feet and ankles that is generally associated with periods of prolonged sitting or standing. The edema is not complicated by manifestations of congestive heart failure or lymphatic disease. The cause of heat edema is muscular and cutaneous vasodilation combined with venous stasis. Interstitial fluid then accumulates in the lower extremities. Because the problem is self-limited, treatment involves use of support hose and simple elevation of the lower limbs. Diuretics are not indicated.
- Caused by peripheral pooling of the intravascular volume
- Patient responds promptly to rest, cooling, and rehydration
Simple fainting may occur suddenly after exertion in the heat. Cutaneous and muscular vasodilation redistributes intravascular volume to the periphery of the body. Volume loss and prolonged standing (pooling in the lower extremities) also contribute to the development of inadequate central venous return and insufficient cerebral perfusion. The patient’s skin is cool and moist, the pulse is weak, and transient hypotension occurs. In general, core temperature is normal or mildly elevated. The patient usually responds promptly to rest in a recumbent position, cooling, and oral rehydration. Evaluate elderly people who experience syncopal episodes for hypoglycemia, arrhythmias, and fixed myocardial or cerebrovascular lesions.
- Spasms of the voluntary muscles of the abdomen and extremities
- Caused by salt depletion
- Treatment consists of fluid and salt replacement
Heat cramps are due primarily to salt depletion and manifested by painful spasms of the voluntary muscles of the abdomen and extremities. The skin may be moist or dry, and cool or warm. Muscle fasciculations may be present. The core temperature is normal or only slightly elevated. Laboratory studies (rarely indicated) may reveal hemoconcentration and low serum sodium levels, although this is variable, and normal serum sodium levels are frequently noted. Hypokalemia occurs occasionally.
Treatment includes oral fluid and salt replacement with 0.1–0.2% salt solution (¼–½ teaspoon table salt in one cup water) or, in severe cases, intravenous normal saline solution. Give supplementary potassium as dictated by measured serum levels. Replace glucose if needed. An alternative therapy for mild symptoms is a commercial electrolyte solution (eg, Gatorade). Place the patient in a cool place, and massage sore muscles gently.
The patient should rest for 1–3 days, depending on the severity of the attack. Hospitalization is usually not required.
- Caused by either primary water loss or primary sodium loss due to prolonged heat exposure
- Rapidly leads to heat stroke
- Symptoms of dehydration are present, but central nervous system symptoms are not seen
- Treatment includes rehydration and cooling
Heat exhaustion is a systemic reaction to prolonged heat exposure (hours to days) and is due to sodium depletion, dehydration, accumulation of metabolites, or a combination of these factors. It is a premonitory syndrome that rapidly evolves to heat stroke. Central nervous system symptoms are generally not present, and the core body temperature is usually less than 40°C (104°F).
Two types of heat exhaustion have been described: hypernatremic (primary water loss) and hyponatremic (primary sodium loss). Heat exhaustion from primary water loss occurs when an individual in a hot environment is denied access to water. Heat exhaustion from primary salt loss occurs when an individual in a hot environment sweats excessive amounts and replaces fluid losses with pure water. It differs from heat cramps in that systemic symptoms are present. Pure forms of either type are rare, and most cases have a mixed salt and water depletion. The signs and symptoms of heat exhaustion are nonspecific and include headache, nausea, vomiting, malaise, muscle cramps, and dizziness. Dehydration is manifested by tachycardia, hypotension, and diaphoresis. In a hypernatremic patient, the water deficit can be calculated by a formula if the current serum sodium and patient’s weight and age are known.
Measurement of serum electrolytes and renal function is advisable in most patients, because serum sodium concentration may be markedly low in patients with heat exhaustion. Myoglobinuria indicates subclinical rhabdomyolysis.
Initial treatment includes placing the patient in a cool place and giving adequate cool water and salted (<200 mOsm/L) fruit drinks or salt tablets according to the estimated amount of water and salt depletion. If the patient is unable to drink fluids, give normal saline or lactated Ringer’s supplementation intravenously in accordance with clinical and laboratory findings. If marked hyponatremia with water intoxication is present, administration of intravenous hypertonic saline may be required (Chapter 43).
Hospitalize patients with moderate to severe symptoms and those who are elderly or have comorbid illnesses.
- Extremely high body temperatures causing altered mental status and multiorgan dysfunction
- Rhabdomyolysis and severe hepatic damage occur
- Treatment is rapid reduction in body temperature
Heat stroke is caused characterized by dysfunction of the heat regulating mechanism, with altered mental status (ranging from confusion to coma) and elevated core body temperature in excess of 41°C (105.8°F). Sweating is variable. The extremely high body temperature rapidly causes widespread damage to body tissues, with significant rhabdomyolysis and multiorgan dysfunction. Illness and death result from destruction of cerebral, cardiovascular, hepatic, and renal tissue.
Heat stroke usually follows excessive exposure to heat and/or strenuous physical activity under exceptionally hot environmental conditions, although it may develop in elderly, infirm, or otherwise susceptible individuals in the absence of unusual exposure to heat. Cardiovascular disease, diabetes, cystic fibrosis, alcoholism, obesity, recent febrile illness, and debility are predisposing factors. Anesthetics, paralyzing agents, diuretics, sedatives, antidepressants, and anticholinergic drugs may also be contributing factors.
Premonitory findings include headache, dizziness, nausea, diarrhea, and visual disturbances. Most patients have profound central nervous system dysfunction including seizures, delirium, and coma. The skin is hot, flushed, and usually dry (although sweating may be present). Prior to cardiovascular collapse, the pulse may be strong and rapid due to an increase in cardiac output with no change in stroke volume. Blood pressure is initially elevated or unchanged, and hypotension is a late finding that signals circulatory collapse. Hyperventilation may cause initial respiratory alkalosis, which is generally followed by metabolic acidosis. Stigmata of coagulopathy may be present and include hematuria, hematemesis, bruising, petechiae, and oozing at sites of venipuncture. Core body temperatures as high as 46°C (114.8°F) have been reported in some patients who have achieved full recovery.
Laboratory findings include hemoconcentration, decreased blood coagulation, and evidence of disseminated intravascular coagulation. Hypoprothrombinemia, hypofibrinogenemia, or thrombocytopenia may be present. The white blood cell count is routinely elevated. Hypophosphatemia and hypokalemia sometimes occur. Hyperkalemia is associated with acute renal failure due to rhabdomyolysis. The patient has scantly concentrated urine (“machine oil urine”) containing protein, tubular casts, and myoglobin. A consistent finding in patients with heatstroke is severe hepatic injury. Serum transaminase levels rise to tens of thousands, although complete recovery usually ensues if treatment is initiated quickly.
Act quickly to prevent further damage. The most critical objectives of treatment are rapid cooling and cardiovascular support.
Maintain an adequate airway and ventilation; monitor arterial blood gas levels. Give supplemental oxygen, 6–10 L/min, by mask or nasal cannula.
Reduce body temperature promptly. As a first-aid measure, place the patient in a shady, cool place and remove his or her clothing. Sprinkle the patient’s entire body with water, and cool by fanning. Alcohol sponge baths are contraindicated and can result in alcohol toxicity. If the victim is near a cold stream, it may be helpful to immerse the patient in the water to facilitate cooling.
In the emergency department, place the patient on a cooling blanket, and place ice packs on the axilla, posterior neck, and inguinal areas (do not apply ice directly to the skin). Water should be sprayed on the patient with a fan blowing on him or her to maximize evaporative cooling. If the temperature cannot be rapidly lowered, or if the victim is unresponsive and the initial core temperature exceeds 42°C (107.6°F), begin peritoneal lavage with cold potassium-free dialysate, 2 L every 10–15 minutes. If a patient requires dialysis, then extracorporeal blood cooling is possible during dialysis. This is also possible via cardiopulmonary bypass, which is a rarely used but extremely effective option. When the rectal temperature drops to 39°C (102.2°F), discontinue active measures to lower temperature to avoid hypothermia, but continue temperature monitoring. Hyperthermia may recur due to thermoregulatory instability, and additional cooling may be required.
Benzodiazepines may be given as needed to control shivering. Because the hypothalamic set point is not elevated as it is in fever, aspirin and acetaminophen have not been found to be helpful. They may even worsen coagulopathy and liver damage.
Maintain adequate urinary output (30–50 mL/h). Insert an indwelling urinary catheter to monitor urine output. If myoglobinuria is present, rehydrate the patient with isotonic saline, alkalinize the urine with intravenous administration of bicarbonate, and consider the use of mannitol, 0.25 g/kg intravenously, to promote diuresis. Maintain blood pressure and urine output with intravenous infusion of crystalloid solutions and inotropic agents as necessary (monitoring of central venous pressure or pulmonary capillary wedge pressure may be required). α-Adrenergic drugs are contraindicated because they produce vasoconstriction and decrease heat exchange. Dobutamine may be preferable to dopamine as an inotropic agent, because it does not have the α-adrenergic renal effects associated with dopamine at rapid rates of infusion.
Hospitalize all patients whose core temperature has exceeded 41°C (105.8°F) for treatment of possible complications (disseminated intravascular coagulation, renal failure, hepatic failure, rhabdomyolysis, cardiac arrhythmias, myocardial infarction, and coma).
With early diagnosis and proper care, 80–90% of previously healthy patients should survive. Extreme hyperpyrexia (rectal temperature >42°C [107.6°F]), persistent coma after cooling, markedly elevated alanine aminotransferase (serum glutamic pyruvic transaminase) and aspartate aminotransferase (serum glutamic oxalacetic transaminase) levels, and hyperkalemia associated with extensive rhabdomyolysis are unfavorable prognostic signs.
Emergency Treatment of Electrical Injuries
- Lightning injuries can result not only in burns but also in multiorgan dysfunction
- Respiratory arrest is the most common cause of death; ventricular fibrillation and asystole are also seen in severe cases
- Management is the same as that for a person with blunt trauma
The United States National Weather Service estimates approximately 60–100 deaths in the United States and 24,000 deaths worldwide due to lightening strikes annually. A reported 30% mortality and 70% morbidity is noted. Epidemiology centers in the mountainous states and the southeastern United States. Strike events cluster in the summer months and in the mid-afternoon, with 84% of victims being male. Injuries are caused by a direct strike, splash (ie, from trees, buildings, and fences), step voltage (spreading on ground), upward leaders, and blunt trauma from concussive shockwaves.
Suspect lightning injury in a person found dazed, unconscious, or injured in the vicinity of a thunderstorm. Certain pathognomonic clinical signs help to establish the diagnosis. Victims may appear initially pulseless with mottled extremities due to autonomic dystrophies and sometimes cardiac standstill. Triage of lightning strike victims differs from other multiple casualty scenarios in that the dead appearing are addressed first.
Lightning contact with the body is instantaneous; a flashover phenomenon may channel most of the current along the outside of the body (over the skin) rather than through the victim, as occurs in other types of electrical injury.
Linear burns are first- and second-degree burns that begin at the head and neck and course in a branching pattern down the chest and legs. They tend to follow areas with a heavy concentration of sweat.
Punctate burns are clusters of discrete, circular, partial- or full-thickness burns that form starburst patterns on the skin.
Feathering burns are not true burns but rather cutaneous imprints from electron showers that track through the skin. They create a fernlike pattern with delicate branching. These patterns are also called ferning, keraunographic markings, and Lichtenberg flowers or figures.








