Anatomy and Pathophysiology
Diseases or dysfunction of the neck causes headache when three conditions are met (
17):
1. Implicated cervical structures are pain sensitive.
2. The referral pain pattern from neck to head is physiologically based.
3. The disease or dysfunction is identifiable and verifiable.
Nociceptive cervical structures include (
2) joints, periosteum, and ligaments of the cervical spine; muscles around the cervical spine; cervical nerve roots and nerves; and vertebral arteries (
Table 121-1). Referred pain from these cervical structures to the head is achieved by:
1. C2 sensory root and its extensions, greater and lesser occipital nerves allowing pain referral to the back of the head.
2. Possibly the C1 sensory root (although some authorities believe it to be nonexistent or inconsequential) allowing pain referral to the vertex or frontal head region (
33).
3. Connections between the tentorial branches of the ophthalmic division of the trigeminal nerve and posterior fossa branches of C2 allowing pain referral from C2-innervated structures to the front of the head.
4. The descending spinal tract of the trigeminal nerve, intermingling impulses from the upper cervical segments with those from cranial nerve V and allowing pain referral from these segments to the head (
34). There is no known physiologic basis for cephalic referral of pain originating from cervical segments below C4.
The
cervical causes of headaches are listed in
Table 121-2. Occipital or suboccipital pain can be the presenting complaint in 26% of developmental anomalies of the craniovertebral junction and upper cervical spine, such as basilar invagination, congenital atlantoaxial dislocation, and separate odontoid; in cases such as these, stretching of
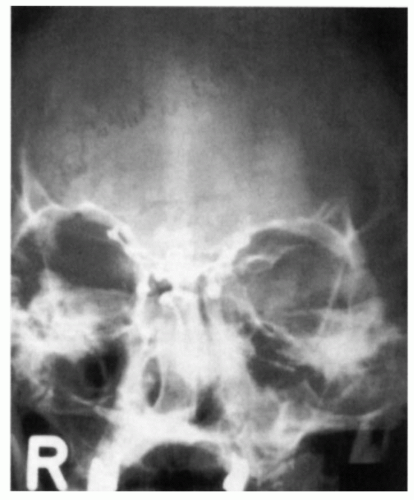
upper cervical nerve roots can be seen at surgery. On the other hand, Klippel-Feil anomaly does not produce head or neck pain unless there is excessive mobility between vertebrae rostral to the congenital fusion, with secondary facet joint changes. Also, cervical spina bifida does not cause headache unless associated with soft tissue anomalies such as Arnold-Chiari malformation, with or without hydrocephalus (
Fig. 121-2).
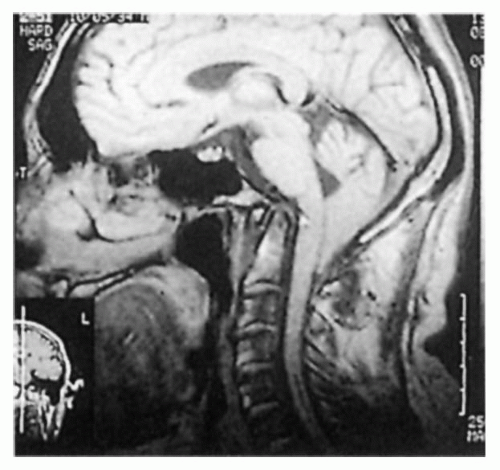
Acquired lesions of the craniovertebral junction and upper cervical spine, such as primary tumors (meningioma, schwannoma, ependymoma), Paget disease of the skull with secondary basilar invagination, osteomyelitis of the upper cervical vertebrae, and multiple myeloma of the skull base or upper cervical vertebrae may produce headache by erosion of the pain-sensitive structures or traction on upper cervical nerve roots (
Fig. 121-3). Blows to the head or even forceful sneezing may produce rotatory subluxation of the atlas, which, through irritation of synovial joints, causes persistent occipital headache. Rheumatoid arthritis of the upper cervical spine produces headaches through a variety of mechanisms, including inflammation of the synovial atlanto-occipital and atlantoaxial joints and stretching of upper cervical ligaments and nerve roots caused by atlanto-axial subluxation secondary to attenuation of the transverse ligament of the odontoid (this also may occur in ankylosing spondylitis).
Cervical spondylosis and
cervical disc disease are not universally accepted to cause headache because they typically involve the lower cervical discs and vertebrae. Also, their almost ubiquitous existence in people over 40 years old makes it difficult to establish causality or even strong association. Restriction of movement in the lower cervical regions may lead to excessive “play” in rostral apophyseal joints (e.g., at C2-C3 or C3-C4), and could cause head pain (
Fig. 121-4), but evidence for this hypothesis remains elusive.
Trauma including “whiplash” injuries is not a widely accepted cause of headache. Clearly, many people with an extension-flexion injury of the neck experience self-limited neck, occipital, and occasionally frontal pain, which clears within days or a few weeks. Likely, this pain results from injury to the upper cervical ligaments and muscles. Others believe that shearing injuries of the long axons in the brainstem and upper cord may disrupt central pain and other regulatory mechanisms, allowing the emergence of headache (
5,
28,
54,
58,
60).
Clinical Features
The IHS diagnostic criteria for cervicogenic headache (
30) (ICHD-II) are as follows:
A. Pain, referred from a source in the neck and perceived in one or more regions of the head and/or face, fulfilling criteria C and D.
B. Clinical, laboratory, and/or imaging evidence of a disorder or lesion within the cervical spine or soft tissues of the neck known to be, or generally accepted as, a valid cause of headache.
C. Evidence that the pain can be attributed to the neck disorder or lesion based on at least one of the following:
1. Demonstration of clinical signs that implicate a source of pain in the neck2
2. Abolition of headache following diagnostic blockade of a cervical structure or its nerve supply using placebo or other adequate control
D. Pain resolves within 3 months after successful treatment of the causative disorder or lesion.
The ICHD-II includes those footnotes or qualifiers to the criteria for cervicogenic headache. These are:
1. Tumors, fractures, infections, and rheumatoid arthritis of the upper cervical spine have not been validated formally as causes of headache, but are nevertheless accepted as valid causes when demonstrated to be so in individual cases. Cervical spondylosis and osteochondritis are NOT accepted as valid causes fulfilling criterion B. When myofascial tender spots are the cause, the headache should be coded under 2. Tension-type headache.
2. Clinical signs acceptable for criterion C1 must have demonstrated reliability and validity. The future task is the identification of such reliable and valid operational tests. Clinical features such as neck pain, focal neck tenderness, history of neck trauma, mechanical exacerbation of pain, unilaterality, coexisting shoulder pain, reduced range of motion in the neck, nuchal onset, nausea, vomiting, photophobia, etc., are not unique to cervicogenic headache. These may be features of cervicogenic headache, but they do not define the relationship between the disorder and the source of the headache.
3. Abolition of headache means complete relief of headache, indicated by a score of 0 on a visual analog scale (VAS). Nevertheless, acceptable as fulfilling criterion C2 is ≥90% reduction in pain to a level of <5 on a 100-point VAS.
While there is nothing specific about headaches from craniovertebral anomalies, they tend to exhibit some suggestive features, such as posterior location, triggering by flexing of the neck or by coughing and straining, and sometimes a pronounced postural component that may mimic low-pressure headaches (
35). Depending on what neural anomalies are associated, there may be complaints of vertigo, facial numbness, limb weakness, or ataxia, as well as neurologic findings related to the upper cervical nerve roots, lower brainstem, or upper cervical cord.
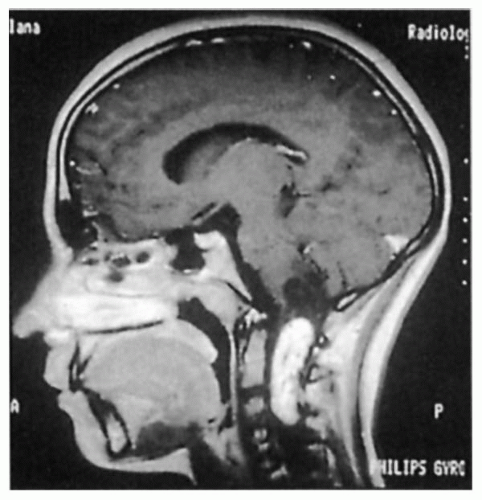
As with the congenital atlantoaxial and upper cervical anomalies, acquired disorders tend to produce occipital headaches that are worsened or triggered by neck movements or straining, although often the postural element of the headache is not so evident (
Fig. 121-5). In addition, aids to diagnosis include the stigmata of the underlying diseases encountered in the history, examination, and investigations. When examining patients with rheumatoid arthritis who have headache, care should be taken when the patient is asked to flex the neck, because occasional fatalities have resulted from compression of the medulla by the odontoid, which, no longer bound to the atlas by the transverse ligament, fails to move away from the brainstem on anteflexion of the cervical spine.
Only gold members can continue reading.
Log In or
Register to continue
Related

Full access? Get Clinical Tree