Chapter 34 Disaster Preparedness, Cardiopulmonary Resuscitation, and Airway Management
V. Hospital Incident Command System
VI. Operating Room Preparation
VII. Anesthetic and Resuscitation Techniques
VIII. Planning and Preparation
IX. Basic Life Support and Cardiopulmonary Resuscitation Guidelines
X. Initial Airway Management During Cardiopulmonary Resuscitation
XI. Advanced Airway Management During Cardiopulmonary Resuscitation
XII. Alternative Methods of Oxygen Delivery During Cardiopulmonary Resuscitation
XIII. Challenges of Airway Management During Cardiopulmonary Resuscitation
I Introduction
Disasters happen. They happen frequently, but they are not uniformly distributed in time and geography. Any particular place tends to experience them infrequently. Although there are many definitions of disaster, the most common medical definition of a disaster is an “event that results in casualties that overwhelm the health care system in which the event occurs.”1 Typically, disasters degrade the fundamental infrastructure necessary for a viable economy and civil society. This disruption magnifies the impact of the event by widening the gap between needed and available resources (Fig. 34-1).
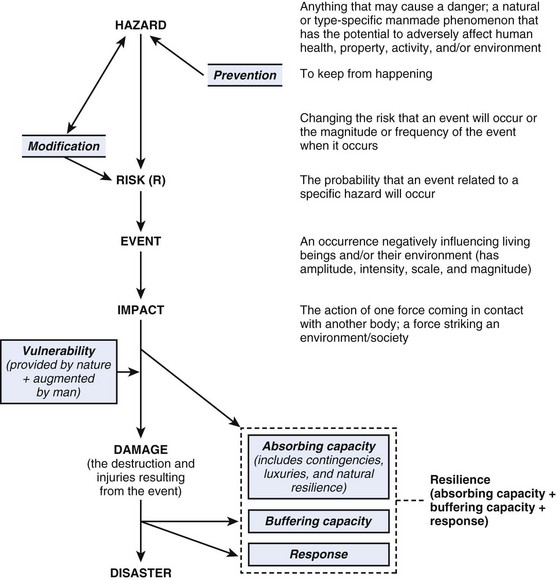
Figure 34-1 Standardized definitions of terms used to communicate by the various disciplines involved in disasters.
(Modified from Task Force for Quality Control of Disaster Medicine (TFQCDM)/World Association for Disaster and Emergency Medicine (WADEM): Health disaster management: guidelines for evaluation and research in the Utstein style, vol 1. Available at http://www.wadem.org/guidelines/chapter_3.pdf [accessed March 2012].)
II Disaster Triage
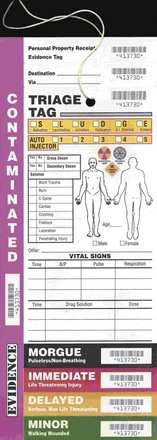
Triage is the act of sorting casualties. It implies that numbers of casualties exceed available medical resources. During routine circumstances in modern hospitals, the sickest patients receive the highest priority. During mass casualty events, patients are sorted into several levels based on the ability to help the greatest number while conserving scarce resources. Several systems are in use, and all are based loosely on military systems but have not been scientifically validated.2 Patients who require intense resources with little likelihood of salvage are called expectant. They are expected to die and are given comfort measures only. Those with severe but treatable conditions are marked as immediate. Wounded who can wait are referred to as delayed or minimal (Fig. 34-2). Because triage depends on resources, repeat triage should occur when there is a change in patient status, available care, and transfer to another facility.
III Surge Capacity
The concept of surge capacity is important beyond the emergency department. As the number of arriving patients peaks, the ability to expand services and number of beds is critical. Although temporarily increased capacity can result from cancellation or delay of routine patient load, there ultimately must be an expansion of overall facility capacity or introduction of new facilities into the system.3 This can be done by adding portable facilities, recruiting administrative space within the institution, or using municipal buildings (e.g., schools) for treatment space. Unless providers and supplies can be augmented from outside the disaster zone, creative allocation of resources is the only option. The Agency for Healthcare Research and Quality (AHRQ) has developed an online, disaster-specific hospital surge model that can be used for planning.4
IV Altered Standards of Care
In large-scale disasters, an altered standard of care must be implemented. Chronic diseases such as diabetes, hypertension, and hypothyroidism become uncontrolled as the medication supply is depleted. Life-threatening conditions such as coronary ischemia and dialysis-dependent renal failure can no longer be treated adequately. Scarce resources are more appropriately directed to others. Loss of sanitation and hygiene increase the frequency of wound infection, respiratory diseases and gastrointestinal diseases. Acute shortages of antibiotics can become a major limitation, and determination of the standard of care can be set regionally (e.g., in pandemic influenza) or done on an ad hoc basis.5
V Hospital Incident Command System
All U.S. hospitals are required by The Joint Commission (TJC), formerly the Joint Commission on Accreditation of Healthcare Organizations (JCAHO), and by governmental policies to have disaster plans prepared and tested twice per year. The most accepted standard for hospital disaster response is the Hospital Incident Response System (HICS) (http://www.hicscenter.org/index.php [accessed March 2012]). HICS consists of a command and control framework headed by the incident commander and prioritized task lists for each designated subordinate. Modeled on military combat systems and perfected by the California Fire Service, HICS is a time-tested system.
VI Operating Room Preparation
On notification of a disaster situation, the local institution’s operating room disaster standard operating procedure should be used.6 HICS does not delineate how a surgical service should organize the operating room. The HICS model should be used with a single chief of the operating room, preferably a senior anesthesiologist who is in communication with the emergency department, intensive care units, postanesthesia care unit, the chief of perioperative nursing, and the hospital’s surgical chief.
VII Anesthetic and Resuscitation Techniques
A Emergency Airway Management and Ventilation
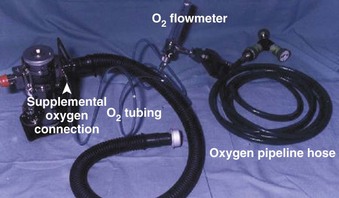
Tracheal intubation, except when performed blindly, requires a light source and a laryngoscope. Typically, the intubated patient requires controlled ventilation. Use of a surgical airway is rarely indicated, but it remains an option in selected cases. The expenditure of effort and resources for such a patient may not be consistent with the most good for the greatest number, but care should not be denied to a salvageable casualty when time and resources are available. Advanced techniques are only as good as their availability and the skill of the practitioner. Several types of portable ventilators can be used during a respiratory disease pandemic if normal infrastructure (i.e., electrical power and compressed gas) is available. Figure 34-3 shows a portable ventilator.

B Anesthetic Techniques
Choice of anesthetic technique depends on the resources available and the skill of the practitioner. Total intravenous anesthesia (TIVA) with local anesthetic infiltration has been the default option when resources are constrained. Needed quantities of parenteral agents such as ketamine, narcotics, benzodiazepines, propofol, and barbiturates are compact, easy to transport, and easy to store. Judicious infiltration of local anesthetics can provide acceptable conditions for short procedures when used alone. Baker and colleagues7 described three levels of military anesthesia care on the battlefield: sevoflurane inhalation using standard anesthesia machines at the highest level, drawover vaporizers at the intermediate level, and TIVA at the lowest level. Regional anesthesia, particularly nerve blocks placed with a nerve stimulator or ultrasound if available, has enjoyed popularity in war zones and during the 2010 Haiti earthquake.8
The Omeda Universal Portable Anesthesia Complete (U-PAC) drawover anesthesia system (GE Healthcare, Fairfield, CT) has been deployed with the U.S. military. Drawover features include durability, compactness, portability, low capital investment, low operating expense, and no requirement for compressed gas or electricity.9 Components of a drawover system include a vaporizer powered by patient respiration or a self-inflating bag with a one-way valve (Fig. 34-4).
VIII Planning and Preparation
The key to successful management during a disaster is good preparation and planning, which starts with a realistic understanding of the situation. When preparing to meet the needs of a distant event, the response should be tailored to the acute and endemic disease spectrum, climate, degree of infrastructure impairment, and cultural particulars of the affected area. An area with inadequate transportation; total loss of power, water, and sanitation; and tenuous security after a major earthquake has significantly different needs from an area experiencing pandemic influenza (Fig. 34-5). Logistics are always the major limiting factor. Resupply may be uncertain or nonexistent. Local manufacture of substitutes (e.g., boiled linen for sterile dressings) may be the only option. Compressed gas and intravenous fluids are heavy, bulky, and in short supply. Lack of refrigeration limits use of certain pharmaceuticals. Modern sterilization methods may not be available, requiring improvisation. Boiling metal instruments for 15 to 30 minutes renders a high degree of asepsis. After thorough cleaning with soap or detergent, soaking heat-intolerant equipment in common household bleach (i.e., sodium hypochlorite solution) is an excellent means of sterilization, but it tends to degrade many materials after repeated application.
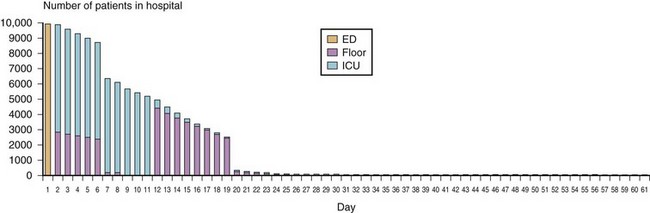
(From U.S. Department of Health and Human Services: Hospital surge model. Available at http://www.hospitalsurgemodel.org [accessed March 2012].)
A The U.S. National Disaster System
The National Incident Management System (NIMS) provides a systematic,10 proactive approach to guide all levels of governmental departments and agencies, nongovernmental organizations, and the private sector to work seamlessly to prevent, protect against, respond to, recover from, and mitigate the effects of incidents, regardless of cause, size, location, or complexity, to reduce the loss of life and property and harm to the environment. NIMS works hand in hand with the National Response Framework (NRF).11 NIMS provides the template for the management of incidents, and the NRF provides the structure and mechanisms for national-level policy for incident management.
The National Disaster Medical System (NDMS) is a nationwide partnership designed to deliver quality medical care to the victims of and the responders to a domestic disaster.12 NDMS provides state-of-the-art medical care under any conditions at the disaster site, in transit from the impacted area, and in participating definitive care facilities.
Related posts:
 Prehospital Airway Management
Prehospital Airway Management
 Medical-Legal Considerations: The ASA Closed Claims Project
Medical-Legal Considerations: The ASA Closed Claims Project
 Ultrasonography in Airway Management
Ultrasonography in Airway Management
 Nonintubation Management of the Airway: Airway Maneuvers and Mask Ventilation
Nonintubation Management of the Airway: Airway Maneuvers and Mask Ventilation

Full access? Get Clinical Tree


