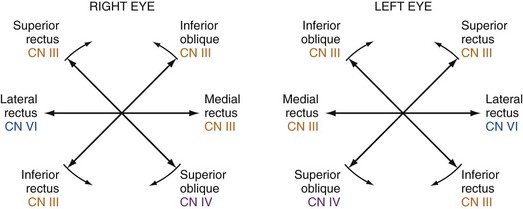
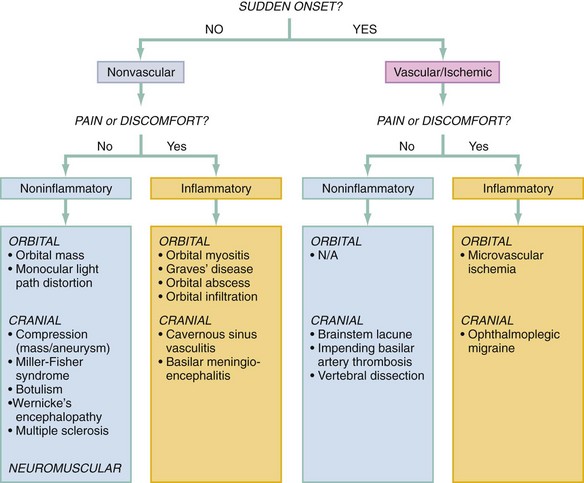
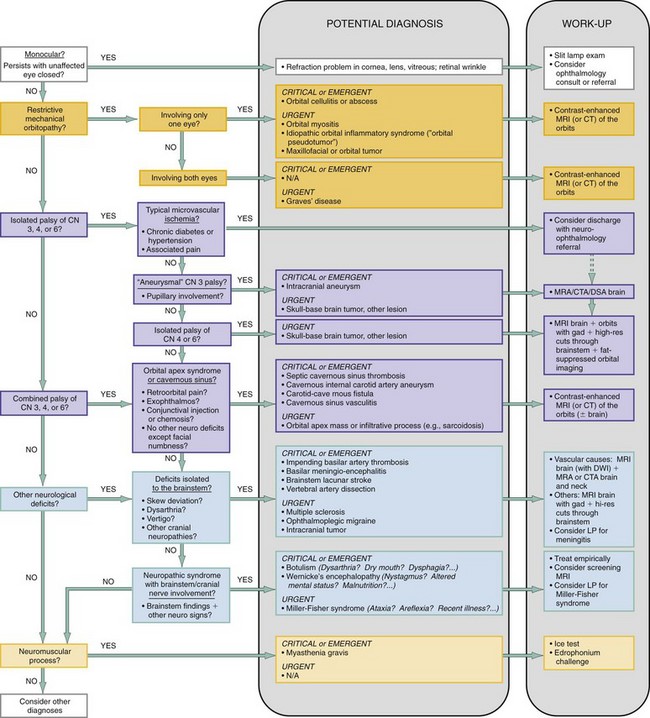
Chapter 21 Diplopia, or double vision, comes in two varieties—monocular and binocular—and constitutes approximately 1.4% of ophthalmologic emergencies. For patients who visit the emergency department (ED) with diplopia, the majority of cases are binocular, with cranial nerve (CN; especially sixth nerve) palsies being among the most common causes.1 The remainder (approximately 15%) are monocular. The refinement of the differential diagnosis for the ED patient with diplopia involves parsing out the exact nature of the diplopia, determining the functional location of the defect, and screening for associated symptoms and findings that may suggest the underlying cause. The majority of this diagnostic resolution is done at the bedside, followed by targeted neuro-ophthalmologic imaging as indicated. The causes of diplopia are myriad, with pathologies relatively benign to relatively fulminant, and the tactical approach to diplopia in the ED entails sorting out those that may result in rapid and profound morbidity from those that are less acute. Table 21-1 outlines some key causes of diplopia prioritized by immediate acuity, with mechanism and distinguishing features. Table 21-1 There are four aspects of questioning that guide the formulation of the differential diagnosis: (1) the cadence of onset and symptoms, (2) the directionality and orientation of the diplopia, (3) the presence of pain, and (4) the presence of other associated symptoms.2,3 In terms of the cadence of onset, a truly sudden onset suggests an ischemic cause, either cerebrovascular or microvascular, especially if the intensity or degree of diplopia was maximal at onset. A fluctuation of symptoms over time may suggest transient ischemic attacks or an impending stroke but also generally implies a neuromuscular disease.2,3 Regarding the directionality of the diplopia, the directions of gaze that elicit or worsen the diplopia, and the general orientation of that diplopia—that is, horizontal, vertical, or torsional—should be carefully determined in order to localize the problem. Finally, symptoms associated with the diplopia (such as pain or neurologic or neuromuscular symptoms) are critical to forming a differential diagnosis, if not to making the diagnosis. The presence of pain suggests an inflammatory or infectious process and narrows the differential significantly. The patient complaining of diplopia should undergo a thorough neurologic examination with attention to the CNs and an evaluation of the six cardinal movements of gaze. Each extraocular muscle (and the nerve that supplies it) has a maximal action in a specific direction, and the evaluation of gaze should therefore specifically follow the configuration of a six-limbed asterisk, or an H2 (Fig. 21-1). The patient should also undergo a careful pupillary and facial examination for signs of pupillary asymmetry, ptosis, lid lag, conjunctival injection or chemosis, periorbital swelling, or proptosis2 and assessment of overall head positioning. The acuity of onset and presence or absence of pain can be used to prestratify diagnostic possibilities as shown in Figure 21-2, especially with regard to vascular, potentially ischemic events. Through use of the lines of questioning and examination elements outlined previously, the differential diagnosis can then be rapidly winnowed down by means of a phased, systematic approach that incorporates the following queries (reflected in the algorithm in Figure 21-3): 2. Is the binocular diplopia a result of a restrictive, mechanical orbitopathy? 3. Is the binocular diplopia a result of a palsy of the oculomotor CNs (III, IV, or VI) in a single eye? 4. Is the binocular diplopia a result of a neuroaxial process involving the brainstem and related CNs? 5. Is the binocular diplopia a result of a neuromuscular disorder? The first key assessment is to determine if the diplopia is purely monocular. Monocular diplopia is an ophthalmologic problem related to distortions in the light path from dry eyes, a corneal irregularity, cataract, or lens dislocation,3,4 or rarely to retinal wrinkles involving the macula.5 The patient with monocular diplopia may require a slit-lamp, funduscopic examination and evaluation by an ophthalmologist and will not typically require an extensive neuro-ophthalmologic workup. Symptoms.: If the patient reports that the diplopia persists in the affected eye with the normal eye closed, this immediately suggests a monocular cause. If the diplopia is determined to be monocular, the evaluation essentially ends with the previous question. If the diplopia is determined to be binocular, on the other hand, the next question is whether or not there is a simple mechanical orbitopathy in one of the orbits causing the diplopia. This type of orbitopathy can be caused by orbital myositis, trauma, or infection (abscess) or by craniofacial masses, any of which can cause direct restriction of the movement of a single eye. Orbital myositis may involve as little as a single extraocular muscle and may be a manifestation of a variety of steroid-responsive conditions, such as Wegener’s granulomatosis, giant cell arteritis, systemic lupus erythematosus, dermatomyositis, sarcoidosis, rheumatoid arthritis, or idiopathic orbital inflammatory syndrome (orbital pseudotumor).7 If both eyes are involved, then thyroid disease (Graves’ orbitopathy) is a consideration. It is the most common cause of ocular myopathy in older adults and is bilateral in at least 85% of cases.9 The patient with thyroid-related diplopia will likely have a preexisting diagnosis of Graves’ disease but may have isolated diplopia before the onset of systemic symptoms (and diagnosis).9 Symptoms.: A structural restriction of motion of a single eye, typically gradual in onset, may cause diplopia in a single or multiple directions of gaze, depending on the type and extent of muscular involvement. A sensation of mass effect, discomfort, or pain in the culprit eye is a characteristic symptom. If the cause is infectious, the patient may describe subjective fever. Diplopia that is worse in the morning suggests Graves’ myopathy, which is presumably worsened owing to the venous congestion of the ocular muscle associated with being supine.2
Diplopia
Perspective
Diagnostic Approach
DIPLOPIA-CAUSING ENTITY
MECHANISM AND MORTALITY
DISTINGUISHING FEATURES
Tier 1—Critical
Basilar artery thrombosis
Acute thrombosis of the basilar artery with brainstem ischemia; untreated, mortality 70-90%
Vertigo, dysarthria, other cranial nerve involvement; risk factors for stroke
Botulism
Toxin inhibits of release of acetylcholine (ACh) at cholinergic synapses and presynaptic myoneural junctions; untreated, mortality 60%
Dysarthria, dysphagia, autonomic dysreflexia, pupillary dysfunction
Basilar meningitis
Infection; untreated, mortality close to 100% if bacterial (25-40% if treated)
Headache, meningismus, fever
Aneurysm
Enlarging aneurysm directly compresses cranial nerve; untreated, rupture risk is 1% per year; mortality 26-50% per rupture
CN III palsy with pupillary involvement
Tier 2—Emergent
Vertebral dissection
Dissection causes vertebrobasilar ischemia; acute untreated, mortality 28% (2-5% if neurologically asymptomatic)
Neck pain, vertigo; risk factors for vertebral dissection
Myasthenia gravis
Autoantibodies develop against ACh nicotinic postsynaptic receptors; untreated, crisis mortality 42% (5% if treated)
Fluctuating muscle weakness, ptosis, and diplopia worsen with activity and improve with rest
Wernicke’s encephalopathy
Thiamine-dependent metabolic failure and tissue injury; untreated, mortality 20%
Nystagmus, ataxia, altered mental status, and ophthalmoplegia; risk factors and nutritional deficiency
Orbital apex syndrome, cavernous sinus process
Inflammation or infection in the orbital apex or cavernous sinus directly affects oculomotor cranial nerves; acute mortality low unless infectious and complicated by meningitis
A combination of palsies of CN III, IV, or VI, with retro-orbital pain, conjunctival injection, and possible periorbital or facial numbness
Tier 3—Urgent
Brainstem tumor
Tumor involvement at the supranuclear level; acute mortality low (long-term mortality variable)
Skew deviation vertical diplopia, internuclear ophthalmoplegia
Miller-Fisher syndrome
Autoantibodies develop to a cranial nerve ganglioside, GQ1b; acute mortality low if fully differentiated from GBS; mortality 2-12% if GBS
Ophthalmoplegia, ataxia, areflexia
Multiple sclerosis
Demyelinating lesions; acute mortality low
Internuclear ophthalmoplegia
Thyroid myopathy (Graves’ disease)
Autoimmune myopathy; acute mortality low with regard to ocular complaints
Proptosis, restriction of elevation and abduction of the eye, signs of Graves’ disease
Ophthalmoplegic migraine
Inflammatory cranial neuropathy; low mortality—self-limited disease
Ipsilateral headache, CN (usually III) palsy
Ischemic neuropathy
Microvascular ischemia; mortality low—self-limited disease
Isolated CN palsy (pupil-sparing if CN III)
Orbital myositis, pseudotumor
Autoimmune or idiopathic myositis; acute mortality low with regard to ocular complaints
Eye pain, restriction of movement, periorbital edema; exophthalmos and chemosis when more severe
Orbital apex mass
A tumor, infiltration, or mass effect in the orbital apex or cavernous sinus directly compresses oculomotor cranial nerves; acute mortality low
A combination of palsies of CN III, IV, or VI, and possible periorbital or facial numbness, with retro-orbital pain, proptosis, signs of venous congestion
Important Historical Elements
The Examination
The Diagnostic Approach
1 Is the Diplopia Monocular?
2 Is the Binocular Diplopia a Result of a Restrictive, Mechanical Orbitopathy?

Full access? Get Clinical Tree


Diplopia
Only gold members can continue reading. Log In or Register to continue



