![]() Clinical suspicion of joint dislocation
Clinical suspicion of joint dislocation
![]() Incidence of dislocations: Dorsal proximal interphalangeal (PIP) >> volar PIP >> dorsal metacarpal (MCP) thumb > dorsal MCP finger >> volar MCP dorsal distal interphalangeal (DIP) >> volar DIP
Incidence of dislocations: Dorsal proximal interphalangeal (PIP) >> volar PIP >> dorsal metacarpal (MCP) thumb > dorsal MCP finger >> volar MCP dorsal distal interphalangeal (DIP) >> volar DIP
![]() Radiographic evidence of dislocation
Radiographic evidence of dislocation
CONTRAINDICATIONS
![]() Complex dislocation—rupture of or entrapment in the joint of ligaments or tendons surrounding the joint requires open reduction and repair
Complex dislocation—rupture of or entrapment in the joint of ligaments or tendons surrounding the joint requires open reduction and repair
![]() Chronic dislocation (>3 weeks duration)
Chronic dislocation (>3 weeks duration)
![]() Open dislocation
Open dislocation
![]() Unstable joint
Unstable joint
![]() Multiple failed reduction attempts can convert a simple dislocation into a complex dislocation and prompt urgent orthopedic consult
Multiple failed reduction attempts can convert a simple dislocation into a complex dislocation and prompt urgent orthopedic consult
![]() General Basic Steps
General Basic Steps
![]() Neurovascular examination
Neurovascular examination
![]() Prereduction radiograph
Prereduction radiograph
![]() Analgesia
Analgesia
![]() Reduction
Reduction
![]() Postreduction neurovascular examination
Postreduction neurovascular examination
![]() Immobilization
Immobilization
![]() Postreduction radiograph
Postreduction radiograph
LANDMARKS
![]() Nerves run on the lateral surface of each digit at the 2, 4, 8, and 10 o’clock positions
Nerves run on the lateral surface of each digit at the 2, 4, 8, and 10 o’clock positions
![]() Flexor tendons run on the volar surface of the digit
Flexor tendons run on the volar surface of the digit
![]() Extensor tendons run on the dorsal surface of the digit
Extensor tendons run on the dorsal surface of the digit
![]() PIP joint
PIP joint
![]() Dorsal dislocation: The fibrous volar plate resists dorsal dislocations (FIGURE 68.1)
Dorsal dislocation: The fibrous volar plate resists dorsal dislocations (FIGURE 68.1)
![]() Complex dislocation: Head of proximal phalanx or ruptured volar plane can become entrapped in the joint space (FIGURE 68.2)
Complex dislocation: Head of proximal phalanx or ruptured volar plane can become entrapped in the joint space (FIGURE 68.2)
![]() Volar dislocation: Three bands of the extensor tendon (central slip, radial and ulnar lateral bands) resist volar dislocations (FIGURE 68.3)
Volar dislocation: Three bands of the extensor tendon (central slip, radial and ulnar lateral bands) resist volar dislocations (FIGURE 68.3)
![]() Complex dislocation: Extensor slip tendons can rupture and become entrapped within the joint space (FIGURE 68.4)
Complex dislocation: Extensor slip tendons can rupture and become entrapped within the joint space (FIGURE 68.4)
![]() Lateral dislocation: Radial collateral ligaments resist ulnar dislocation, ulnar collateral ligaments resist radial dislocation
Lateral dislocation: Radial collateral ligaments resist ulnar dislocation, ulnar collateral ligaments resist radial dislocation
![]() DIP and thumb IP: Mechanisms of dislocation and reduction are anatomically analogous
DIP and thumb IP: Mechanisms of dislocation and reduction are anatomically analogous
RISKS/CONSENT ISSUES
![]() Risks in joint reduction include swelling with permanent joint enlargement, residual pain, stiffness, or deformity and conversion into complex dislocation including fracture
Risks in joint reduction include swelling with permanent joint enlargement, residual pain, stiffness, or deformity and conversion into complex dislocation including fracture
![]() Risks in anesthesia
Risks in anesthesia
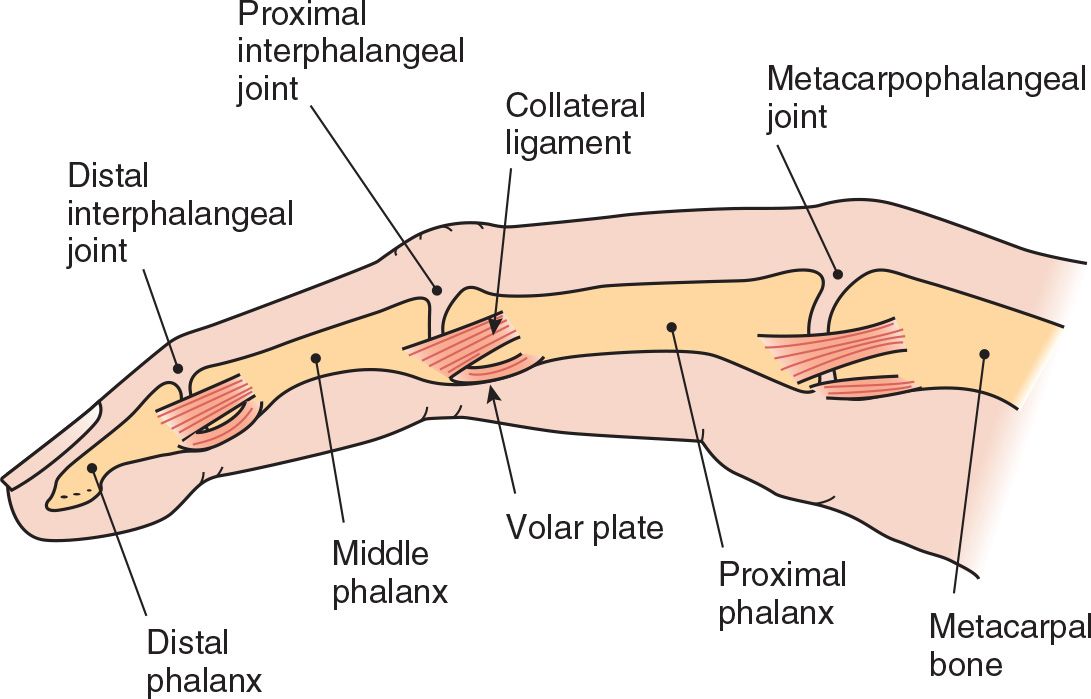
FIGURE 68.1 Fibrous volar plates are found at the MCP and IP joints where they reinforce the joint capsules and limit hyperextension. (From Leggit, JC, Meko CJ. Acute finger injuries: Part I. Tendons and ligaments. Am Fam Physician. 2006;73(5):810–816.)
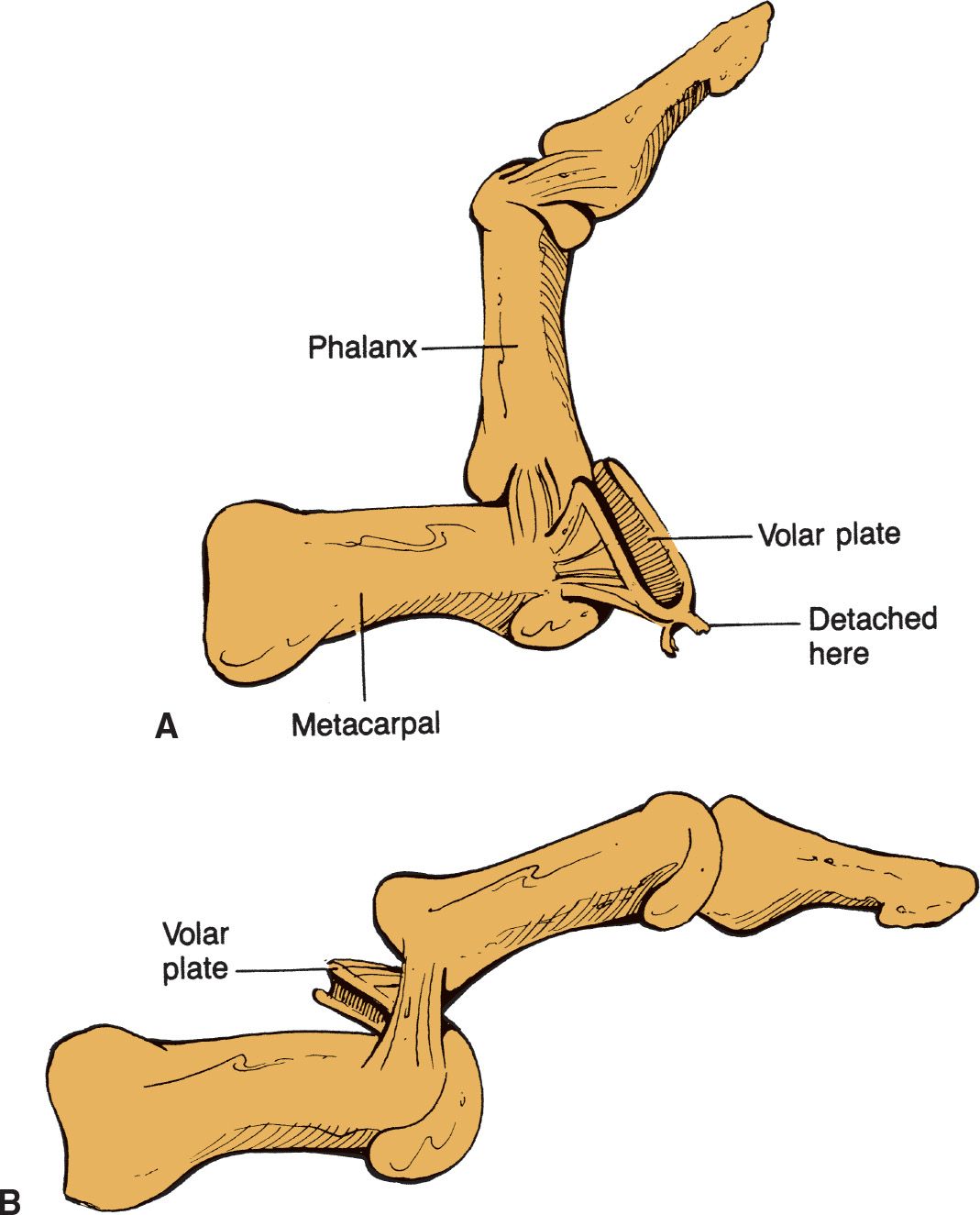
FIGURE 68.2 Complex dorsal PIP dislocation indicated by (A) rupture of PIP volar plate and (B) entrapment of volar plate fibers and head of proximal phalanx into the joint space. (Jackimczyk K, Shepherd SM, Blackburn P. Hand injuries. In: Wolfson AB, ed. Harwood-Nuss’ Clinical Practice of Emergency Medicine. 5th ed. Philadelphia, PA: Williams & Wilkins; 2009, with permission.)
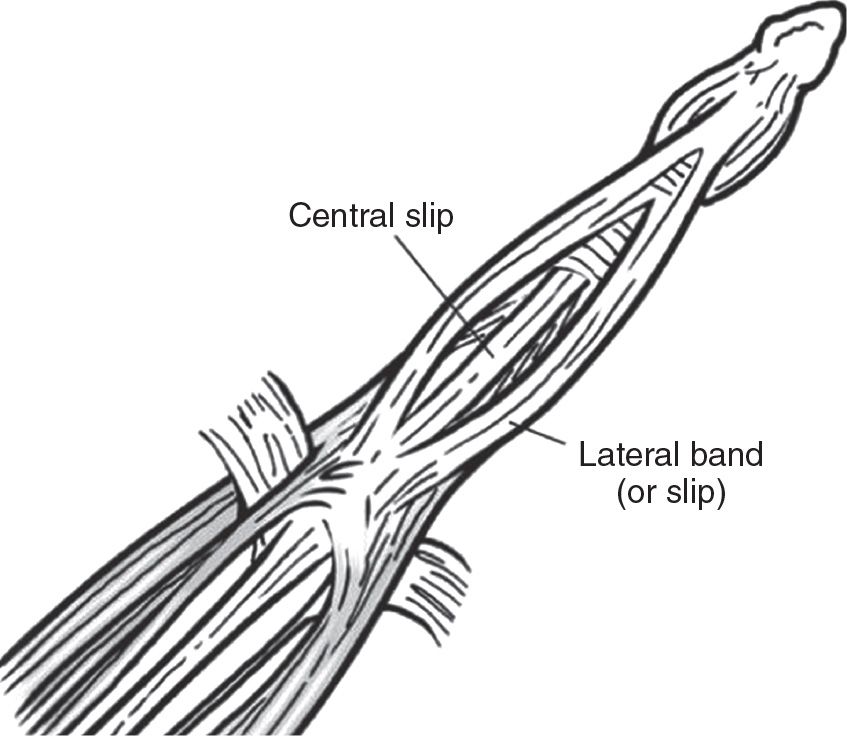
FIGURE 68.3 Extensor tendon mechanism trifurcates at the dorsum of the proximal phalanx (Reichman EF. Emergency Medicine Procedures. 2013. Permission pending.)
SUPPLIES
![]() Anesthesia
Anesthesia
![]() Reduction: 3″ Webril or gauze padding, 3″ plaster roll, 3″ Ace bandage, aluminum finger splint, adhesive tape, scissors
Reduction: 3″ Webril or gauze padding, 3″ plaster roll, 3″ Ace bandage, aluminum finger splint, adhesive tape, scissors
NEUROVASCULAR EXAMINATION
Any deficit indicates a complex dislocation and urgent orthopedic consultation
![]() Inspection
Inspection
![]() Exclude open dislocation
Exclude open dislocation
![]() Complex dislocation presents with less angulated deformities, with skin dimpling, or rotational deformity of the involved phalanges
Complex dislocation presents with less angulated deformities, with skin dimpling, or rotational deformity of the involved phalanges
![]() Palpation—frank fracture fragments
Palpation—frank fracture fragments
![]() Sensation—normal two-point discrimination on finger pad is between 2 to 4 mm
Sensation—normal two-point discrimination on finger pad is between 2 to 4 mm
![]() Vascular—radial and ulnar pulse-Doppler signal
Vascular—radial and ulnar pulse-Doppler signal
![]() Range of motion with stress—assess joint stability with the finger in full extension and in moderate flexion. If displacement occurs, the joint is unstable.
Range of motion with stress—assess joint stability with the finger in full extension and in moderate flexion. If displacement occurs, the joint is unstable.
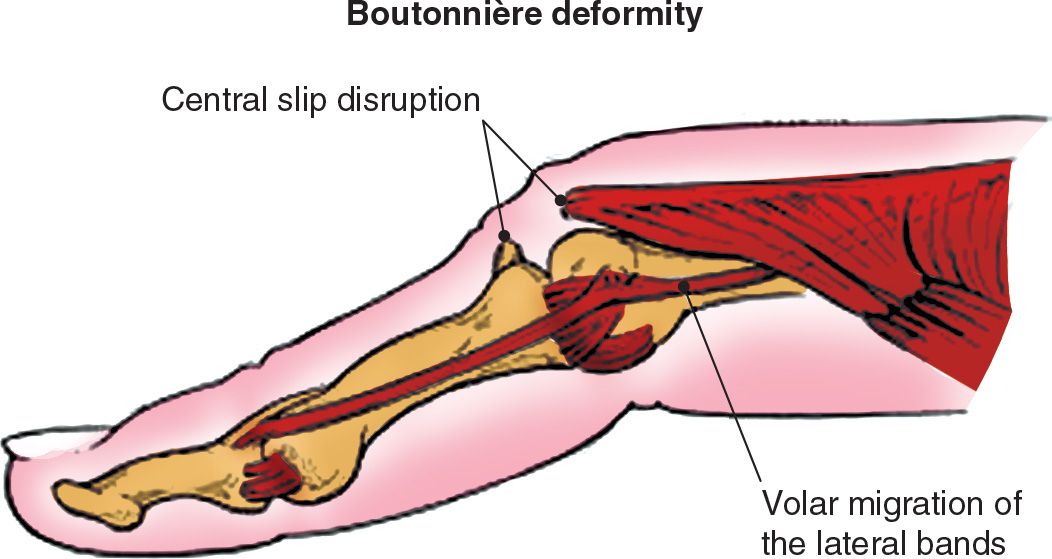
FIGURE 68.4 Central slip of the extensor tendon can rupture in sudden IP hyperflexion and can require operative repair. (From Leggit JC, Meko CJ. Acute finger injuries: Part I. Tendons and ligaments. Am Fam Physician. 2006;73(5):810–816.)

Full access? Get Clinical Tree


