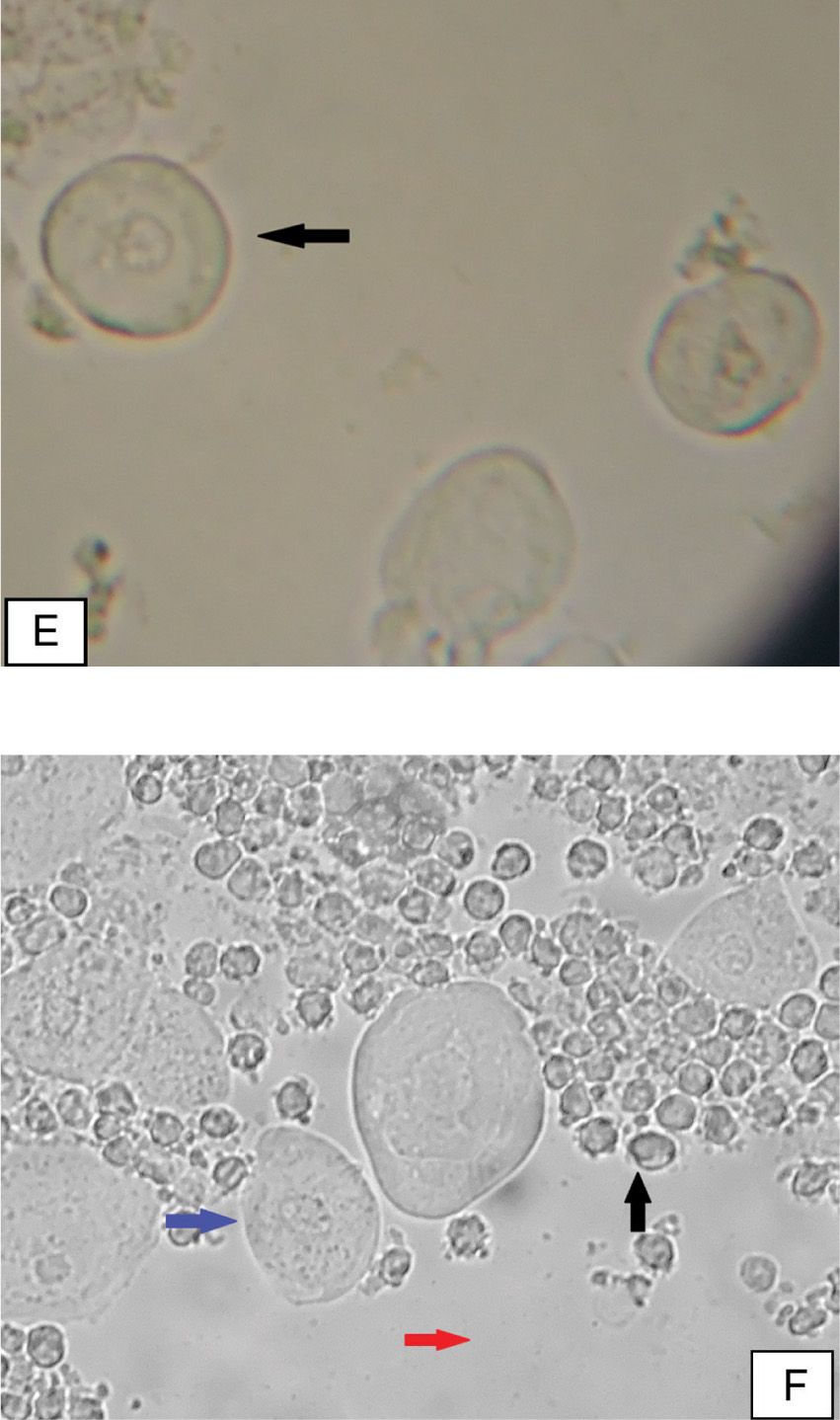
FIGURE 1 Microscopic findings of vaginal conditions
A-Normal wet mount: Mature squamous epithelial cells (black arrow), appear as large, polygonal cells. There is one or no white blood cell (blue arrow) per epithelial cell, and gram-positive rods (lactobacillus morphotypes) (red arrow) are present. This wet mount represents normal discharge, and is accompanied with normal pH (≤4.5).
B-Bacterial vaginosis (BV): clue cells (black arrow) are mature squamous epithelial cells, with adherence of abnormal bacteria to the cell. The flora is comprised of abnormal coccid bacteria (red arrow), without elevation of inflammatory cells.
C-Yeast Infection: Mature squamous epithelial cells (black arrow), rod bacteria suggestive of lactobacilli (blue arrow), hyphae (purple arrow) and budding yeast (red arrow). The specific species cannot be recognized from the smear, and a culture is required for identification.
D- Trichomoniasis: wet mount reveals an increase of inflammatory cells (blue arrow) and parabasal cells (black arrow). The parasites Trichomonas vaginalis are ovoid-shaped and slightly larger than inflammatory cells (red arrow), and they are best recognized by their motility.
E-Vaginal atrophy: characteristic findings are the presence of parabasal cells (black arrow), which are smaller, rounder, and have a large nucleus compared to mature squamous epithelial cells, with scanty vaginal flora as well as an elevated pH (>4.5).
F-Desquamative inflammatory vaginitis (DIV): microscopic findings show high number of white blood cells (black arrow), an increase of immature, parabasal epithelial cells and intermediate epithelial cells (blue arrow), an absence of lactobacilli and a coccoid flora (red arrow). The pH is>4.5.
Contact Dermatitis
Contact dermatitis (CD) is an inflammation of the skin due to exposure to an exogenous agent acting as a primary irritant or an allergen. As vulvar tissue is susceptible to irritants, CD is common and can complicate all other vulvovaginal conditions. As symptoms are of nonspecific inflammation, diagnosis is based on detailed history, exclusion of infectious causes, and a high level of suspicion.
Lichen Sclerosus
Lichen sclerosus (LS) is a chronic, inflammatory skin disorder affecting 0.1–1.7% of women [12]. Classic findings include hypopigmentation, epithelial thinning or thickening, and hemorrhages. LS causes scarring of vulvar tissue, loss of normal architecture, including disappearance of labia minora, clitoral adhesions and narrowing of the introital opening. It may affect vulvar and perianal areas with the classic “figure 8” appearance or only small areas of skin. Typically, there is no vaginal involvement.
Lichen Planus
Lichen planus (LP) [31] is a systemic inflammatory mucocutaneous disorder which can involve the vagina, vulva, and vestibule. The most common variant is erosive LP, causing painful vestibular erosion that appears as deep glazed erythema. It can cause vaginitis or localized erosive lesions in the vagina. The inflammatory process can cause adhesions, fibrosis, and even complete vaginal obliteration. Introital stenosis and destruction of normal vulvar architecture can occur.
Classic LP presents with white, reticulate, lacy striae. Diagnosis is based on either physical examination findings or biopsy.
Genital Pain Syndromes: Provoked Vulvar Pain Syndrome /ProvokedVestibulodynia (PVPS/PVD) and Generalized Vulvar Pain Syndrome/ Generalized Unprovoked Vulvodynia (GVPS/GVD)
Patients with VP, in whom there is not another recognized disorder, are diagnosed with vulvar pain syndrome (VPS)/vulvodynia. The IASP and ISSVD terminology for classification of VPS/vulvodynia distinguishes between generalized and localized pain, and each of these two subgroups is further subdivided into provoked, unprovoked, or mixed (continuous pain, exacerbated by touch) [32]. The majority of presentations are either provoked VPS/provoked vestibulodynia, formerly known as vulvar vestibulitis syndrome, or generalized VPS/generalized unprovoked vulvodynia.
PVPS/PVD
PVPS/PVD is a syndrome of provoked, localized allodynia of the vulvar vestibule, not explained by another condition, which lasts more than 3 months. PVPS/PVD was first described as a syndrome in 1987 by Dr. Friedrich [14] and was termed vulvar vestibulitis syndrome. Friedrich’s criteria were: (1) severe pain in the vulvar vestibule upon touch or attempted vaginal entry; (2) tenderness to pressure localized within the vestibule; and (3) erythema of various degrees.
As inflammation is often not found, the term vestibulitis was dropped in 2003 by the ISSVD and the name was changed to PVD [32]. The diagnostic criteria remain similar to those suggested by Friedrich and include typical history of pain upon vestibular touch, such as attempted intercourse, gynecological examination, tampon insertion or other direct contact, and a suitable Q tip test which elicits severe pain or discomfort. Most patients with PVPS/PVD present with dyspareunia or a complete inability to have intercourse.
GVPS/GVD
GVPS/GVD replaced the older terminology, dysesthetic vulvodynia, essential vulvodynia, and burning vulva syndrome [32]. Patients report a continuous unpleasant pain sensation, usually burning, stinging, irritating, itching, or a feeling of rawness. Most often pain is diffuse, without clear borders. Any stimulus which results in pressure on the vulva can exacerbate the pain, including intercourse, tight fitting clothing, sitting, walking, or exercising.
DESCRIBING THE SUBJECT
Causes of Provoked Vulvar Pain Syndrome/Provoked Vestibulodynia (PVPS/PVD)
There is a belief that PVPS/PVD represents a group of distinct disorders that have been classified together simply because they produce pain in the same anatomic location [23]. Causes of these disorders include hormonal imbalance, caused mainly by hormonal contraception [7,18,21,27], nerve fiber proliferation in the vestibular mucosa, [5,6,43,44] and hyperactive pelvic floor (PF) dysfunction [37,45]. PVPS/PVD may appear with first attempts of sexual intercourse or tampon insertion (primary PVPS/PVD) or can be a new onset of pain with activities that did not illicit pain in the past (secondary PVPS/PVD) [46].
Studies found that various factors such as genetic, inflammatory mediators, recurrent vaginitis, allergy, and trauma may be involved in the development of PVPS/PVD.
A high percentage of VP patients report an antecedent history of recurrent or intractable candida vulvovaginitis, although it is unknown if this represents a true increase in incidence or an original misdiagnosis. It has been suggested that repeated vulvovaginitis is a triggering event for some women leading to chronic VP. This observation has led to hypothesis that in a patient with neurogenic vulnerability, an initiating event or series of events may lead to chronic VP [11,19,47].
Several studies point to a possible genetic involvement with polymorphisms in genes responsible for regulating inflammatory response: allele 2 of the IL-1b gene[16], mannose-binding lectin (MBL)[2], melanocortin-1 receptor (MC1R) gene[13], and the gene coding for the inflammasome component NALP3 [30]. The theory suggests that some women with PVPS/PVD have defective regulation of proinflammatory immune responses, due to genetic variations that predispose them to exaggerated inflammatory responses [15,16,30,47]. Chronic inflammation may induce changes to peripheral nociceptors or may represent an increased exaggerated neurogenic inflammation, facilitating central sensitization.
Because the diagnosis of VPS/vulvodynia is nonspecific, treatment is not evidence based and proceeds on a trial and error basis. At least 30 different therapeutic interventions have been suggested for the management of VPS/vulvodynia, yet evidence from clinical trials remains largely inconclusive [1]. Recommendations are in favor for a multi-disciplinary approach focusing on pain management and re-establishing the PF function [4].
A different approach is suggested by Goldstein[17]. He classifies PVPS/PVD groups, based on history and exam findings:
Hormonally mediated PVPS/PVD – The pain began while taking hormonal contraceptives. Typically, patients have a low calculated free testosterone and complain of dryness, decreased libido and arousal. The entire vestibule is tender and vestibular mucosa is often dry and thin. Treatment includes stopping hormonal contraception and application of topical estradiol (± testosterone) to the vestibule [9].
Hyperactive pelvic muscle dysfunction – PF muscles become tight and tender. Patients often have other symptoms suggesting hyperactivity (see below) and predisposing factors, such as musculoskeletal disorders or anxiety, may coexist. Typically, the pain is much worse at 4–8 o’clock position of the vestibule with minimal or no pain in the upper vestibule. Treatment includes PF physiotherapy, with an optional addition of muscle relaxants (diazepam suppositories), Botulinum toxin injections and cognitive behavioral therapy.
Neuroproliferative PVPS/PVD – Women have an increased number of nociceptors in the vestibular mucosa. This group is further subdivided into congenital and acquired forms. In the congenital subgroup, vestibular pain has always been present, and there may be sensitivity to palpation of the belly button, due to common embryologic origin (the primitive urogenital sinus)[10]. With acquired neuroproliferative PVPS/PVD, the pain began after a severe allergic reaction or vaginitis. There is tenderness of the entire vestibule. Treatments include topical anaesthetics, antidepressants, antiseizure drugs, capsaicin cream and vestibulectomy.
As with PVPS/PVD, the term generalized VPS/generalized unprovoked vulvodynia describes a symptom, the question is whether we can diagnose a specific cause instead of calling it simply “vulvar pain”. It is possible that some cases of GVPS/GVD may represent a pudendal nerve disorder, PF hyperactive disorder, or can be classified as an entity within the spectrum of neuropathic pain syndromes, while in other patients it represents functional pain syndrome.
PRACTICAL IMPLICATIONS
Assessment of Patients with Genital Pain




Full access? Get Clinical Tree


