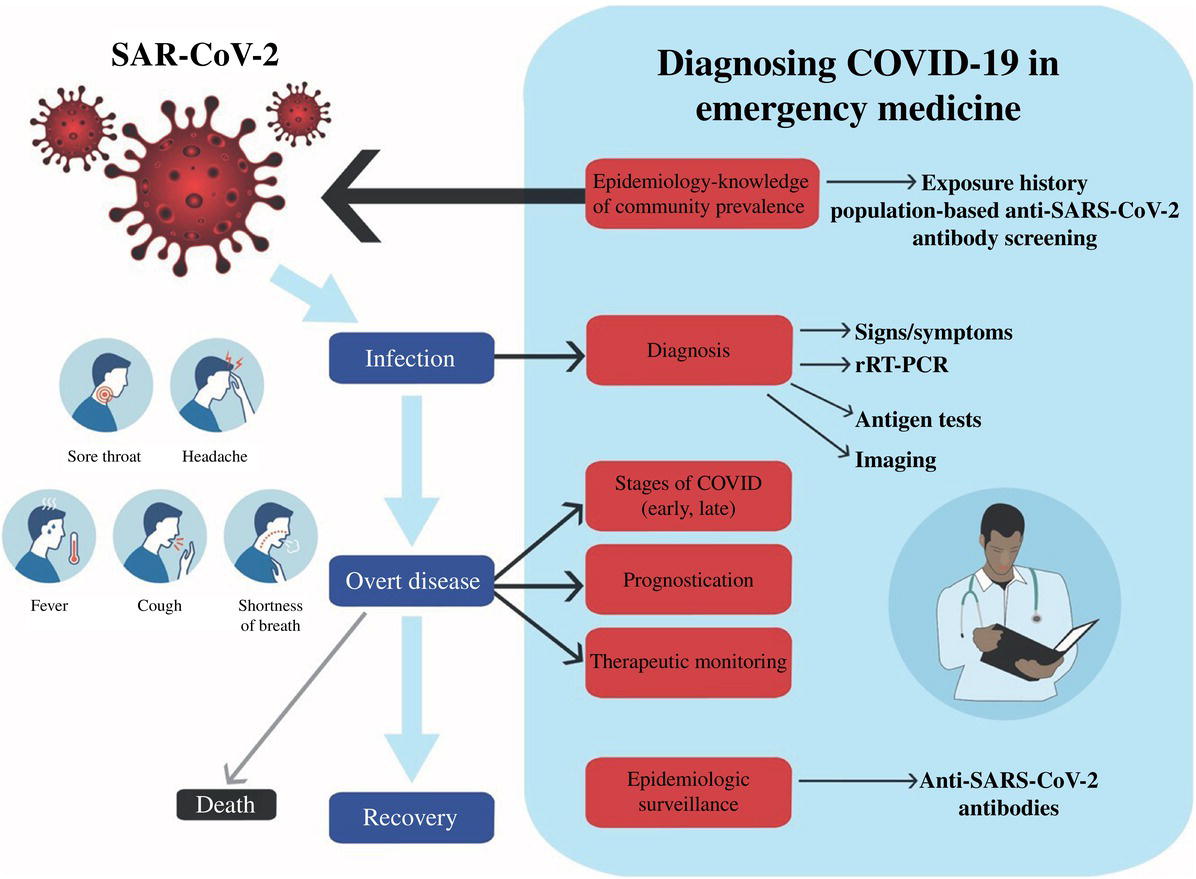
Christopher R. Carpenter1 and Jesse M. Pines2,3 1 Department of Emergency Medicine, Washington University School of Medicine, St. Louis, MO, USA 2 US Acute Care Solutions, Canton, OH, USA 3 Department of Emergency Medicine, Drexel University, Philadelphia, PA, USA A novel viral respiratory pathogen emerged in December 2019 called severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2) with the corresponding illness called coronavirus disease (COVID‐19). COVID‐19 became a potentially life‐threatening viral infection for a significant portion of the population and millions of people died worldwide during the 2 years. The global pandemic catalyzed economic stress and exposed geopolitical divisions, while scientists grappled with emerging diagnostic, prognostic, and therapeutic approaches at an unprecedented pace. Amidst the backdrop of this generational catastrophe, the existential foundations of evidence‐based medicine described in Chapters 2 and 3 were challenged as never before with a rush to reporting at a pace that created an accelerating avalanche of unreviewed or inadequately peer‐reviewed research and placed an increased onus on clinicians to display healthy skepticism and concomitant clinical agility.1 Before the science of COVID‐19 prognosis or therapeutics could evolve, accurate and readily available diagnostic tests were required. In February 2020, the United States Food and Drug Administration issued an emergency use authorization (EUA) enabling Centers for Disease Control‐qualified labs to perform COVID‐19 testing. Over 100 EUAs were issued for commercial COVID‐19 assays over the next year as the emergency department (ED) served simultaneously as a societal safety net for routine emergencies, a rapid testing and disposition site, and a lynchpin for epidemic surveillance (Figure 62.1).2 While clinicians managed intermittent waves of symptomatic and asymptomatic exposed patients amidst a sea of diagnostic and management recommendations and protocols that changed frequently, decision‐making was further complicated by shortages of personal protective equipment and test assays. Figure 62.1 Diagnosing COVID‐19 in the ED requires awareness of exposure history and symptom duration. Test results can guide both diagnosis and prognosis. COVID‐19 testing can also be used as a screening test for patient clustering during admission to reduce hospital spread. (Reproduced from [2]/With permission of John Wiley & Sons.) Can clinical signs and symptoms or routine labs accurately distinguish COVID‐19 from other respiratory viral infection? An emergency medicine‐focused diagnostic scoping review in the early months of the pandemic identified few studies quantifying the accuracy or reliability of history and physical exam for diagnosing COVID‐19.2 Few studies reported sensitivity or specificity and none adhered to the Standards for Reporting of Diagnostic Accuracy (STARD) reporting standards for history and physical exam.3 Hypogeusia (positive likelihood ratio [LR+] 7.1, negative likelihood ratio [LR−] 0.38) and hyposmia (LR+ 5.3, LR− 0.61) better ruled in COVID‐19 than ruled out the diagnosis.4 Subsequently, a Cochrane diagnostic accuracy systematic review identified studies evaluating 27 signs and systems categorized as general, respiratory, gastrointestinal, and cardiovascular.5 In general, signs and symptoms had higher specificity and sensitivity of less than 50%. Therefore, COVID‐19 infections often present with different constellations of symptoms, rather than having a classic clinical presentation. The five findings with sensitivity greater than 50% and LR+ >5 in at least one study included fever, myalgia or arthralgia, fatigue, and headache. Studies that examined clinical features enrolled hospitalized patients or patients presenting to the hospital rather than presumably healthier outpatient cohorts. Therefore, spectrum bias likely increased observed sensitivity as discussed in Chapter 6.6 Both the Cochrane review and the emergency medicine scoping review concluded that signs and symptoms alone were inadequate to rule in or rule out COVID‐19 – and that future history/physical exam research needed to adhere to STARD guidelines.2,5 The inaccuracy of history/physical exam alone to rule in or rule out COVID‐19 in the ED suggests that in scenarios with clinician suspicion for SARS‐CoV‐2 based on epidemiological grounds (i.e., high population prevalence or community test positivity rate), adopting a liberal testing strategy is preferred to detect a high proportion of infections in clinical settings. A separate Cochrane review evaluated 21 studies that included 14,126 COVID‐19 patients and 55,585 non‐COVID‐19 patients that quantified the diagnostic accuracy of 67 labs routinely available in most hospitals.7 Only three of the labs had summary sensitivity and specificity over 50%: increase in interleukin‐6, increase in C‐reactive protein, and lymphocyte count decrease (Table 62.1). Other tests based on low‐certainty evidence demonstrated less accuracy, including white blood cell count, increase neutrophil percentage, decrease platelet count, liver function tests, and procalcitonin. None of these labs are sufficient to rule in or rule out COVID‐19. Table 62.1 Routine labs with highest accuracy for COVID‐19 Source: Data from [7]. Which COVID‐19 molecular or antigen test most accurately diagnoses the presence or absence of SARS‐CoV‐2? Real‐time reverse transcription polymerase chain reaction (rRT‐PCR, a molecular test) has become the criterion standard for the presence or absence of COVID‐19 across clinical and imaging studies. The rRT‐PCR tests provide a qualitative detection of SARS‐CoV‐2 nucleic acid. In the United States, the CDC‐developed rRT‐PCR detects two separate regions of the SARS‐CoV‐2 nucleocapsid gene (N1 and N2) with the virus considered present (a positive test) when amplification of both N1 and N2 are detected and absent when neither N1 nor N2 is detected. An inconclusive test represents detection of only one nucleocapsid gene. False‐negative rRT‐PCR results are common, so clinicians and researchers using this test as a criterion standard should include patient’s exposure risk, epidemiological risk based on community prevalence, and clinical and imaging findings when interpreting the accuracy of this result. Unfortunately, most early COVID‐19 diagnostic studies did not incorporate these factors when reporting rRT‐PCR results. Table 62.2 provides common causes of false‐negative rRT‐PCR results.2 COVID‐19 test samples in the ED were most commonly nasopharyngeal, but oropharyngeal sputum sampling is about 3% less sensitive.8 Blood and urine are inadequate specimens for rRT‐PCR because SARS‐CoV‐2 is not present in those body compartments.9 Table 62.2 Common causes of false negative rRT‐PCR Source: Reproduced from [2]/With permission of John Wiley & Sons. RNA = ribonucleic acid; NP = nasopharyngeal; OP = oropharyngeal; BAL = bronchoalveolar lavage. Table 62.3 Comparative accuracy of antigen and rRT‐PCR for COVID‐19 Source: Adapted from [10].
Chapter 62
Diagnosing COVID‐19
Background
Clinical question
Lab
Number of studies
Summary sensitivity (%)
Median specificity (%)
Level of certainty
Interleukin‐6
4
73
58
Very low
C‐reactive protein
14
66
44
Very low
Lymphocyte count
13
64
53
Low
Clinical question
Lab handling (heat inactivation)
Limit of detection (RNA particle detection)
Mutations in the probe target
Sampling procedure (training, fidelity, patient cooperation)
Selective virus replication (patient variability, disease severity variability)
Specimen sampled (NP, OP, saliva, sputum, BAL, stool)
Test kit quality
Timing of sampling in course of disease
Diagnostic tests
Related posts:

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access




