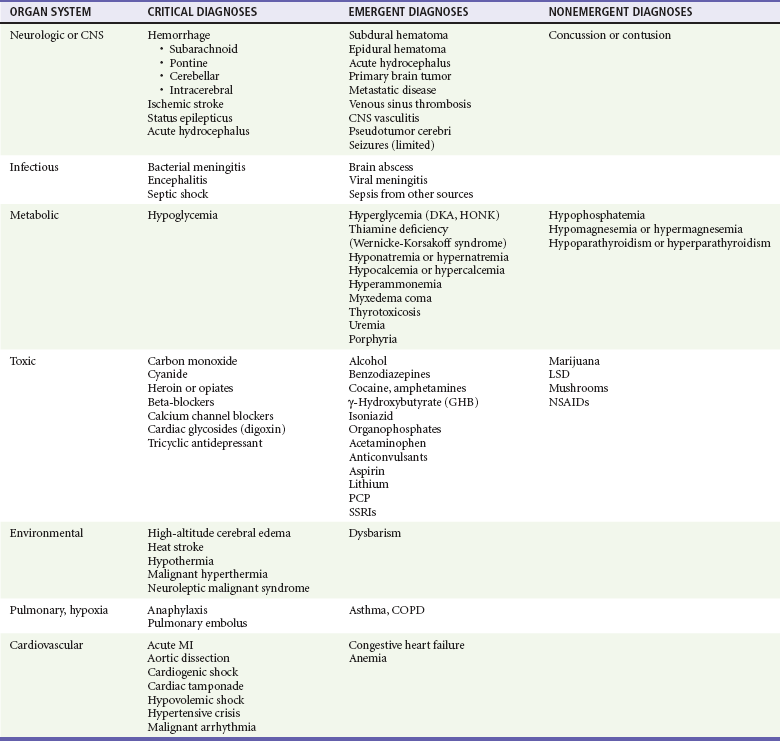
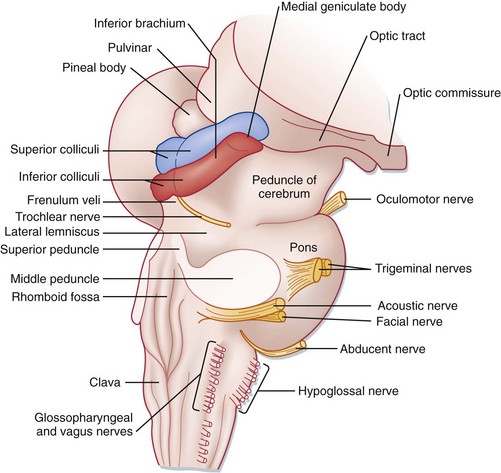
Chapter 16 Depressed mental status represents an alteration in arousal and is a common presenting complaint in the emergency department (ED). This presentation can be the manifestation of a wide spectrum of diseases, with the degree of impairment ranging along a continuum from sleepiness to decreased alertness to frank coma. The differential diagnosis of stupor and coma is broad and diverse (Table 16-1) but can usually be categorized into metabolic and systemic, structural, or psychogenic causes. The majority of cases are caused by metabolic or systemic derangements, whereas the remainder are usually caused by structural lesions. Psychogenic presentations are much less common. The differential diagnosis for depressed level of consciousness often overlaps with that for confusion (see Chapter 17). Frequently, diagnosis and management occur simultaneously, and a structured systematic approach is used. A thorough grasp of the underlying pathophysiology leading to the acute depressed mental state will lead to timely diagnosis and treatment. Table 16-1 The ascending reticular activating system (ARAS) is the neuroanatomic structure primarily responsible for arousal and cortical activation. It is located in the paramedian tegmental zone in the dorsal part of the brainstem (Fig. 16-1). The input of somatic and sensory stimuli to the cerebral cortex is controlled by the ARAS and functions to initiate arousal from sleep. The brain’s cognition centers are located primarily in the cerebral cortex and serve to determine the content of consciousness. Figure 16-1 Brainstem anatomy. (Adapted from Adams J: Emergency Medicine. Philadelphia: Elsevier; 2008.) Head trauma, stroke, tumor, and infection are the most common structural causes of coma and depressed consciousness. Traumatic causes can include subdural and epidural hematomas, intraparenchymal or subarachnoid hemorrhage, or simply contusion or concussion. Strokes occur with embolic, thrombotic, or hemorrhagic mechanisms, but it is extremely unusual for ischemic (i.e., nonhemorrhagic) stroke to depress consciousness unless a massive insult to both hemispheres has occurred (e.g., diffuse severe cerebral edema after a massive infarct) or a high-grade basilar artery stenosis or occlusion is present.1 Depression of consciousness with CNS infections may be caused by mass effect and is common with severe bacterial meningitis, cerebral abscess or empyema, or parasitic mass. Malignancies, whether primary or metastatic, can cause depressed consciousness if the tumor mass elevates intracranial pressure (ICP) or reduces cerebral blood flow, or if surrounding edema develops rapidly. Special consideration should be given to specific populations of patients. The elderly, in particular, are susceptible to alterations in therapeutic medication dosage and drug-drug interactions. Even seemingly minor infections, such as urinary tract infections, upper respiratory infections, or viral gastroenteritis, may cause altered mental status (see Chapter 13), depressed consciousness, or coma. In addition, immunocompromised patients with acquired immunodeficiency syndrome (AIDS) or those undergoing chemotherapy treatments for transplants, and patients with malignancy or immunologic disease are vulnerable to a multitude of opportunistic infections not commonly seen in the general patient population. The clinical evaluation and stabilization of patients with depressed consciousness occur simultaneously with the diagnosis in the ED. The differential diagnosis of depression of consciousness is extensive but can be greatly simplified by focusing attention on the distinguishing characteristics of the available patient history and physical examination (Box 16-1).2 Approaching the patient’s presentation systematically, beginning with a broad differential diagnosis, usually allows development of a short list of likely diagnoses early in the encounter. Often, information from alternate sources guides the diagnostic workup. Common sources of information include family members, neighbors, prehospital personnel, law enforcement, and nursing home staff.3 They may know of preceding symptoms such as headache, nausea, vomiting, or fever. Key historical information includes the rate of symptom onset, a history of trauma, exposure to drugs or toxins, or new medications or change in dosage. Rate of symptom onset is important, as an abrupt onset of decreased alertness may suggest structural phenomena or vascular insult, whereas a gradual onset would be more indicative of the slow, indolent course frequently seen with toxic, metabolic, or infectious causes. Family members usually have some knowledge regarding the patient’s past medical history, which may include diabetes, liver or renal disease, vascular disease such as hypertension, coronary disease, stroke or transient ischemic attacks, malignancy, seizures, immunocompromised states such as human immunodeficiency virus (HIV) infection, sickle cell disease, organ transplantation, or psychiatric illness. Family members may also be able to relay additional diagnostic clues such as rate of onset or waxing-waning characteristics of the patient’s symptoms. In addition, previous medical records should be reviewed whenever possible to augment or confirm the information provided. Items with the patient such as a card in the wallet containing lists of medical conditions and/or medications or a medical alert bracelet or necklace can provide valuable information. If the patient’s historical baseline mental status cannot be established, the current presentation is assumed to be an acute change.4 Causes of depression of consciousness vary with patient age (Box 16-2). The elderly are particularly vulnerable to infectious causes, medication changes, and alterations in their living environments. Young adults and adolescents are more likely to be affected after recreational drug use or trauma. Accidental toxic ingestions are often seen in younger children. In infants, infectious causes of depressed consciousness are most common; however, trauma secondary to physical abuse and metabolic derangements from inborn errors of metabolism can be seen.5
Depressed Consciousness and Coma
Perspective
Pathophysiology
Diagnostic Approach
Pivotal Findings






