CHAPTER 49
Dental Trauma
(Fracture, Subluxation, and Displacement)
Presentation
After a direct blow to the mouth in an accidental fall, motor vehicle collision, sports activity, or fight, a portion of a patient’s tooth (most often one of the maxillary incisors) may be broken off, or a tooth may be loosened to a variable degree.
Ellis class I dental fractures (Figure 49-1) involve only enamel and are a problem only if they have left a sharp edge, which can be filed down with an emery board. Ellis class II fractures (Figure 49-2) expose yellow dentin, which is sensitive to temperature, percussion, and forced air; can become infected; and should be covered. Ellis class III fractures (Figure 49-3) expose pulp that is pink, may bleed, and usually hurt.

Figure 49-1 Ellis class I dental fracture. (From Knoop KJ, Stack LB, Storrow AB: Atlas of emergency medicine. New York, 2002, McGraw-Hill.)

Figure 49-2 Ellis class II dental fracture. (From Knoop KJ, Stack LB, Storrow AB: Atlas of emergency medicine. New York, 2002, McGraw-Hill.)
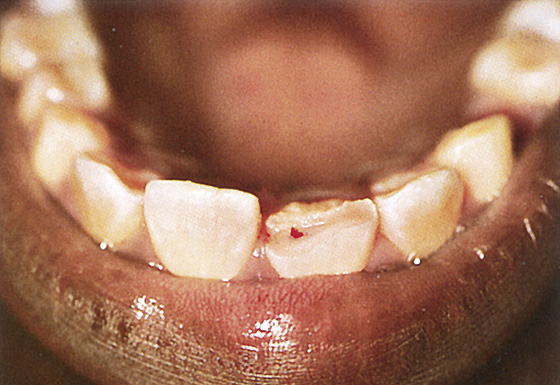
Figure 49-3 Ellis class III dental fracture. (From Knoop KJ, Stack LB, Storrow AB: Atlas of emergency medicine. New York, 2002, McGraw-Hill.)
A tooth that is either impacted inward or partially avulsed outward is recognizable, because its occlusal surface is out of alignment compared with adjacent teeth. There is also usually some hemorrhaging at the gingival margin. If several teeth move together, suspect a fracture of the alveolar ridge. Figure 49-4 shows normal dental anatomy.
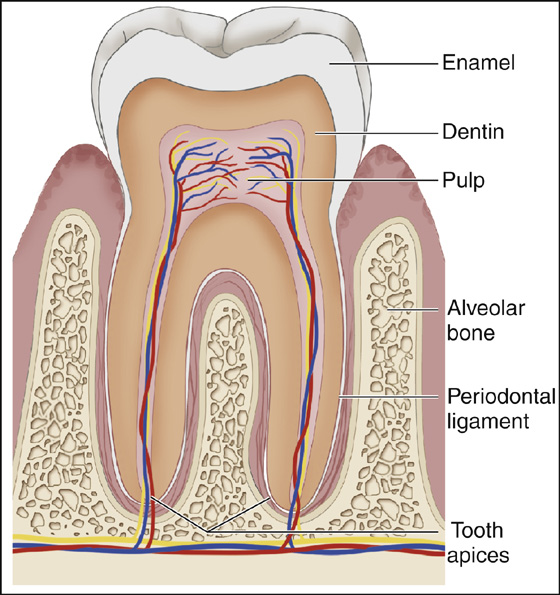
Figure 49-4 Anatomy of the tooth.
What To Do:
 Assess the patient for any associated injuries, such as facial or mandibular fractures. Pay special attention to the temporomandibular joints. Clean and irrigate the mouth to expose all injuries. Touch injured teeth with a tongue depressor, or grasp them between gloved fingers to see if they are loose, sensitive, painful, or bleeding.
Assess the patient for any associated injuries, such as facial or mandibular fractures. Pay special attention to the temporomandibular joints. Clean and irrigate the mouth to expose all injuries. Touch injured teeth with a tongue depressor, or grasp them between gloved fingers to see if they are loose, sensitive, painful, or bleeding.
 Consider possible locations of any tooth fragments. Broken tooth fragments may be embedded in the soft tissue, swallowed, or aspirated. Intraoral wounds should be explored for retained dental fragments. Ultrasonography can be used to detect foreign bodies that may be deeply imbedded and difficult to palpate. A chest radiograph examination can disclose tooth fragments that have been aspirated into the bronchial tree.
Consider possible locations of any tooth fragments. Broken tooth fragments may be embedded in the soft tissue, swallowed, or aspirated. Intraoral wounds should be explored for retained dental fragments. Ultrasonography can be used to detect foreign bodies that may be deeply imbedded and difficult to palpate. A chest radiograph examination can disclose tooth fragments that have been aspirated into the bronchial tree.
 When there is an open wound, provide tetanus prophylaxis as indicated.
When there is an open wound, provide tetanus prophylaxis as indicated.
 For uncomplicated Ellis class I fractures, the patient can be instructed to file the rough edges with an emery board and then to see a dentist for reshaping and polishing the broken tooth or, for larger fractures, providing composite fillings to replace the broken portion.
For uncomplicated Ellis class I fractures, the patient can be instructed to file the rough edges with an emery board and then to see a dentist for reshaping and polishing the broken tooth or, for larger fractures, providing composite fillings to replace the broken portion.
 For sensitive Ellis class II fractures exposing dentin, cover the exposed surface with a calcium hydroxide composition (Dycal), zinc oxide, tooth varnish (copal ether varnish), cyanoacrylate (Dermabond), a strip of Stomahesive, or clear nail polish to decrease sensitivity. Younger patients have less dentin; therefore the pulp is closer to the enamel and is at greater risk for injury and infection. Treat these patients aggressively. Provide pain medications, instruct the patient to avoid hot and cold food or drink, and arrange for follow-up with a dentist the next day. Children should be referred the same day if possible.
For sensitive Ellis class II fractures exposing dentin, cover the exposed surface with a calcium hydroxide composition (Dycal), zinc oxide, tooth varnish (copal ether varnish), cyanoacrylate (Dermabond), a strip of Stomahesive, or clear nail polish to decrease sensitivity. Younger patients have less dentin; therefore the pulp is closer to the enamel and is at greater risk for injury and infection. Treat these patients aggressively. Provide pain medications, instruct the patient to avoid hot and cold food or drink, and arrange for follow-up with a dentist the next day. Children should be referred the same day if possible.
 Patients with Ellis class III fractures exposing pulp should be seen by a dentist immediately (ideally within 3 hours). The tooth should be cleaned, then calcium hydroxide or moist cotton covered with foil be used as a temporary covering. Alternatively, medical-grade cyanoacrylate (Dermabond) can be placed on the exposed pulp to decrease the risk for infection and reduce the pain of an exposed nerve. Provide analgesics as needed.
Patients with Ellis class III fractures exposing pulp should be seen by a dentist immediately (ideally within 3 hours). The tooth should be cleaned, then calcium hydroxide or moist cotton covered with foil be used as a temporary covering. Alternatively, medical-grade cyanoacrylate (Dermabond) can be placed on the exposed pulp to decrease the risk for infection and reduce the pain of an exposed nerve. Provide analgesics as needed.
 Prescribe penicillin (Pen-Vee K), 500 mg qid × 10 days. Use erythromycin or azithromycin in penicillin-allergic individuals. Root canal will have to be performed to avoid dental extraction.
Prescribe penicillin (Pen-Vee K), 500 mg qid × 10 days. Use erythromycin or azithromycin in penicillin-allergic individuals. Root canal will have to be performed to avoid dental extraction.
 Minimally subluxed (loosened) teeth may require no emergency treatment other than a soft diet for 1 to 2 weeks and dental follow-up. Very loose teeth should be pressed back into their sockets (see Chapter 42) and wired or covered with a temporary periodontal splint (Coe-Pak) for stability for up to 48 hours. The patient should be scheduled for dental follow-up, definitive fixation, and a possible root canal. These patients should be placed on a soft food or liquid diet to prevent further tooth motion. Antibiotic prophylaxis with penicillin should be provided (Pen-Vee K), 500 mg qid for 5 to 10 days.
Minimally subluxed (loosened) teeth may require no emergency treatment other than a soft diet for 1 to 2 weeks and dental follow-up. Very loose teeth should be pressed back into their sockets (see Chapter 42) and wired or covered with a temporary periodontal splint (Coe-Pak) for stability for up to 48 hours. The patient should be scheduled for dental follow-up, definitive fixation, and a possible root canal. These patients should be placed on a soft food or liquid diet to prevent further tooth motion. Antibiotic prophylaxis with penicillin should be provided (Pen-Vee K), 500 mg qid for 5 to 10 days.
 Intruded primary teeth and permanent teeth of young patients can be left alone and allowed to re-erupt. Intruded teeth of adolescents and older patients are usually repositioned by an oral surgeon.
Intruded primary teeth and permanent teeth of young patients can be left alone and allowed to re-erupt. Intruded teeth of adolescents and older patients are usually repositioned by an oral surgeon.
 An extruded primary or permanent tooth can be readily returned to its original position by applying firm pressure with your fingers. Both intrusive and extrusive injuries require early dental follow-up and antibiotic prophylaxis, such as penicillin V potassium, 500 mg qid × 10 days (see Chapter 42).
An extruded primary or permanent tooth can be readily returned to its original position by applying firm pressure with your fingers. Both intrusive and extrusive injuries require early dental follow-up and antibiotic prophylaxis, such as penicillin V potassium, 500 mg qid × 10 days (see Chapter 42).
 Inform patients that any trauma to teeth can disrupt the blood supply to a tooth and lead to the eventual need for root canal.
Inform patients that any trauma to teeth can disrupt the blood supply to a tooth and lead to the eventual need for root canal.
What Not To Do:
 Do not fail to consider or recognize domestic abuse and/or child abuse.
Do not fail to consider or recognize domestic abuse and/or child abuse.
 Do not overlook associated injuries of the alveolar ridge, mandible, facial bones, or neck.
Do not overlook associated injuries of the alveolar ridge, mandible, facial bones, or neck.
 Do not use bone wax on complicated crown fractures with exposure of the pulp. It can cause inflammatory reactions.
Do not use bone wax on complicated crown fractures with exposure of the pulp. It can cause inflammatory reactions.
Discussion
Accurately describing the dental anatomy can be very helpful when communicating with your dental consultant. The adult mouth consists of 32 teeth, named from midline to lateral. There is a set of central incisors and lateral incisors, a set of canines (or cuspids), two sets of premolars (or bicuspids), and three sets of permanent molars (first, second, and third molars). The third molars are referred to as “wisdom” teeth.
Each tooth is assigned a number starting with the right maxillary third molar as number 1, ending with the left maxillary third molar as number 16. The number 17 is assigned to the left mandibular third molar and the number 32 to the right mandibular third molar (Figure 49-5).
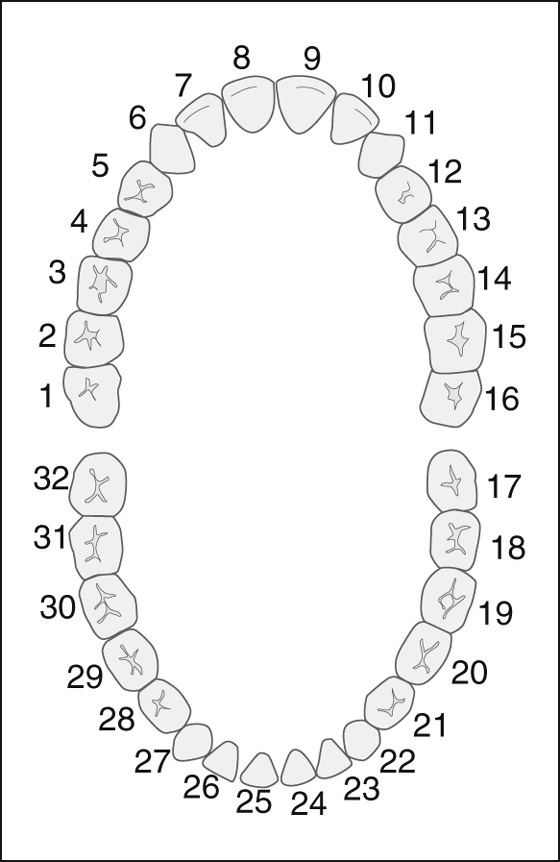
Figure 49-5 Dental map.
Dentists generally no longer use the Ellis system for classifying dental fractures. These fractures can simply be described as being an uncomplicated “enamel fracture” or a fracture with “exposed dentin” or a complicated crown fracture that involves the pulp of the tooth. Exposure of dentin leads to variable sequelae, depending on the age of the patient. Because it is composed of microtubules, dentin can serve as a conduit for pathogenic microorganisms.
In children, the exposed dentin in an Ellis class II fracture lies nearer the neurovascular pulp and is more likely to lead to a pulp infection. Therefore, in patients younger than 12 years of age, this injury requires a dressing such as a calcium hydroxide composition (Dycal). Mix a drop of resin and catalyst over the fracture, and, although unnecessary, if you wish, cover it with dry aluminum foil. When in doubt, consult a dentist. If these fractures are covered quickly, pulpal contamination can be prevented, and subsequent root canal may be avoided.
If a temporary periodontal splint (Coe-Pak) or wire is not available to stabilize loose teeth, spread soft wax over palatal and labial tooth surfaces and neighboring teeth as a temporary splint (see Chapter 42 for additional techniques).
Root fractures are clinically difficult to diagnose; patients may notice abnormal mobility and sensitivity to percussion of the tooth.
Related posts:

Full access? Get Clinical Tree


