Administer a strong analgesic, such as oxycodone in combination with acetaminophen (Percocet, Tylox), and prescribe additional medication, including nonsteroidal anti-inflammatory drugs (NSAIDs), for home use. Severe pain may necessitate a nerve block with a long-acting local anesthetic, such as bupivacaine (Marcaine) 0.5% (see Appendix D).
 If a cavity is present, insert a small cotton pledget soaked in oil of cloves (eugenol). The cotton should fill the cavity loosely without rising above the opening (where it would strike the opposing tooth). An alternative to eugenol is a pearl of benzonatate (Tessalon Perles), opened so that the contents can soak the small cotton pledget. Alternatively, benzonatate pearls can be prescribed, and the patient can bite them for repeated topical anesthesia.
If a cavity is present, insert a small cotton pledget soaked in oil of cloves (eugenol). The cotton should fill the cavity loosely without rising above the opening (where it would strike the opposing tooth). An alternative to eugenol is a pearl of benzonatate (Tessalon Perles), opened so that the contents can soak the small cotton pledget. Alternatively, benzonatate pearls can be prescribed, and the patient can bite them for repeated topical anesthesia.
 Refer the patient to a dentist for definitive therapy (removal of caries, removal of pulp, or removal of the tooth) within 12 hours.
Refer the patient to a dentist for definitive therapy (removal of caries, removal of pulp, or removal of the tooth) within 12 hours.
What Not To Do:
 Do not prescribe antibiotics if there are no signs of cellulitis or visible abscess formation.
Do not prescribe antibiotics if there are no signs of cellulitis or visible abscess formation.
 Do not pack a tooth cavity tightly with eugenol-soaked cotton. If an abscess develops, this cavity may serve as a route for drainage.
Do not pack a tooth cavity tightly with eugenol-soaked cotton. If an abscess develops, this cavity may serve as a route for drainage.
Discussion
Dental decay presents visually as opaque white areas of enamel with gray undertones or, in more advanced cases, as brownish, discolored cavitations. Caries are initially asymptomatic. Pain does not occur until the decay impinges on the pulp and an inflammatory process develops. Reversible pulpitis is mild inflammation of the tooth pulp caused by caries encroaching on the pulp. Pain is triggered by hot, cold, and sweet stimuli; lasts for a few seconds; and resolves spontaneously. Treatment involves removal of the carious tissue and replacement with a dental restoration or filling.
As the patient’s condition progresses from reversible pulpitis to irreversible pulpitis (Figure 48-1) and pulpal necrosis, he experiences excruciating pain caused by fluid and gaseous pressure within a closed space. Heat increases the pressure and pain, whereas cold reduces it. The pain is persistent and is often poorly localized.
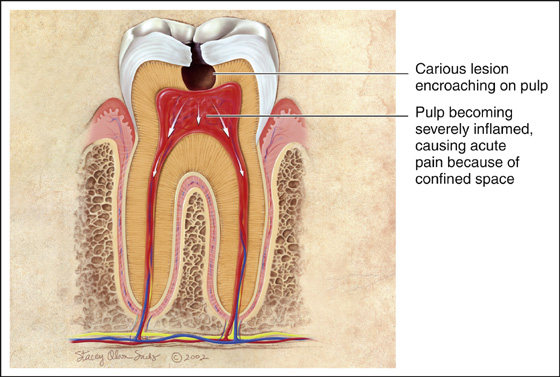
Figure 48-1 Irreversible pulpitis. (From Douglass AB, Douglass JM: Common dental emergencies. Am Fam Physician 67:511-516, 2003.)
Intractable pain usually responds to nerve block techniques with injection of long-acting local anesthetics.
If a patient refuses a nerve block or a nerve block fails to relieve the pain, consider the possibility that the patient is seeking drugs. At the same time, remember that some people have extreme phobias about dental injections. When in doubt, err on the side of compassion.
The only way to definitively treat the discomfort of irreversible pulpitis is root canal treatment (removal of the pulp and filling of the empty pulp chamber and canal) or extraction of the tooth. The urgency of referral to a dentist should be determined by the patient’s level of discomfort, but examination should not be delayed for more than a few days. Patients should be warned to return if they develop signs of cellulitis, such as facial swelling, fever, and malaise.


Full access? Get Clinical Tree


