CHAPTER 45
Dental Pain, Periapical Abscess
(Tooth Abscess)
Presentation
The patient complains of severe, constant facial or dental pain, often associated with facial swelling, regional lymphadenopathy, and cellulitis, and may be accompanied by signs of systemic toxicity. The pain may be gnawing or throbbing or sharp and shooting. Dental caries may or may not be apparent. Percussion of the offending tooth causes increased pain (Figure 45-1). The severe toothache may be exacerbated by thermal changes, especially cold drinks. On the other hand, hot and cold sensitivity may no longer be present because of necrosis of the pulp. A fluctuant abscess may be palpated in the buccal or palatal gingiva, but usually extending toward the buccal side and to the gingival-buccal reflection.
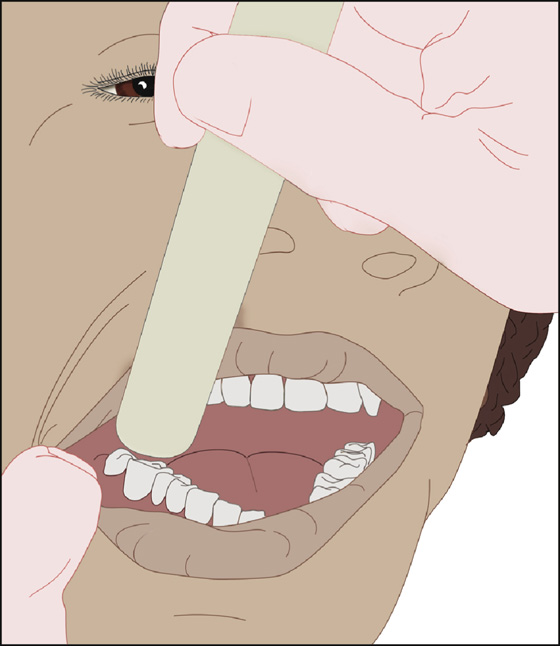
Figure 45-1 Percussion of tooth with tongue blade.
See normal anatomy (Figure 45-2) with subsequent development of periapical abscess and cellulitis (Figure 45-3).
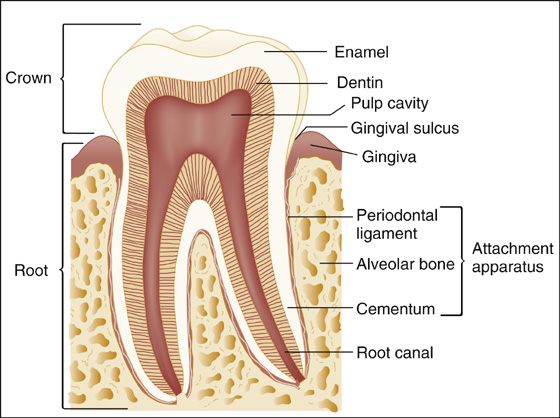
Figure 45-2 Normal tooth anatomy. (From Marx JA, Hockberger RS, Walls RM, et al: Rosen’s emergency medicine concepts and clinical practice, ed 7. Philadelphia, 2010, Mosby.)
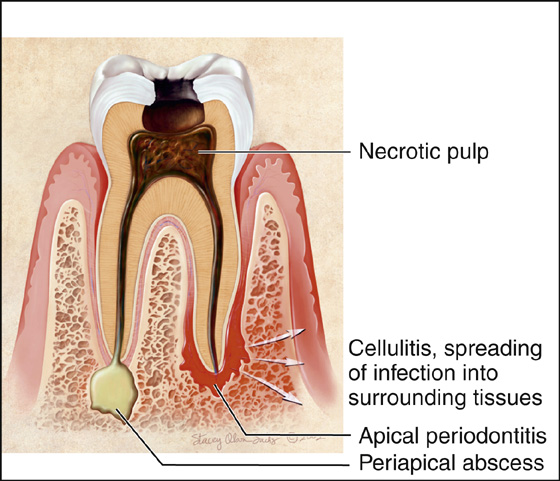
Figure 45-3 Apical periodontitis, periapical abscess, and cellulitis. (From Douglass AB, Douglass JM: Common dental emergencies. Am Fam Physician 67:511-513, 2003.)
What To Do:
 The quickest way to control dental pain is with a dental block. See Appendix D for inferior alveolar or apical nerve block. Use of bupivacaine (Marcaine) as the anesthetic agent will give prolonged pain relief.
The quickest way to control dental pain is with a dental block. See Appendix D for inferior alveolar or apical nerve block. Use of bupivacaine (Marcaine) as the anesthetic agent will give prolonged pain relief.
 Adequate pain medication should be administered and prescribed for continued pain relief until dental follow-up can be arranged. Nonsteroidal anti-inflammatory drugs (NSAIDs) are excellent for dental pain and often suffice or can be administered in combination with narcotic pain medications for synergistic analgesia if necessary. Provide a small prescription for 15 tabs of acetaminophen with hydrocodone or oxycodone (Vicodin or Percocet) to help manage the patient’s pain until he can follow up with a dentist.
Adequate pain medication should be administered and prescribed for continued pain relief until dental follow-up can be arranged. Nonsteroidal anti-inflammatory drugs (NSAIDs) are excellent for dental pain and often suffice or can be administered in combination with narcotic pain medications for synergistic analgesia if necessary. Provide a small prescription for 15 tabs of acetaminophen with hydrocodone or oxycodone (Vicodin or Percocet) to help manage the patient’s pain until he can follow up with a dentist.
 Antibiotics are not necessary to treat apical abscesses unless concurrent cellulitis is present.
Antibiotics are not necessary to treat apical abscesses unless concurrent cellulitis is present.
 When cellulitis and facial swelling are present, depending on the level of toxicity, the patient initially should be treated with either parenteral or oral penicillin. A 10-day course of penicillin VK, 500 mg qid, should be prescribed in adults or 50 mg/kg/day divided into three doses in children. Erythromycin or clindamycin may be substituted if the patient is allergic to penicillin.
When cellulitis and facial swelling are present, depending on the level of toxicity, the patient initially should be treated with either parenteral or oral penicillin. A 10-day course of penicillin VK, 500 mg qid, should be prescribed in adults or 50 mg/kg/day divided into three doses in children. Erythromycin or clindamycin may be substituted if the patient is allergic to penicillin.
 If a fluctuant gingival abscess cavity is present (Figure 45-4), perform incision and drainage at the most dependent location. Provide local anesthesia with 1% lidocaine (Xylocaine) with epinephrine. With gingival swelling and fluctuance, incision and drainage can often be accomplished by sliding a No. 15 scalpel blade between the tooth and gingiva.
If a fluctuant gingival abscess cavity is present (Figure 45-4), perform incision and drainage at the most dependent location. Provide local anesthesia with 1% lidocaine (Xylocaine) with epinephrine. With gingival swelling and fluctuance, incision and drainage can often be accomplished by sliding a No. 15 scalpel blade between the tooth and gingiva.
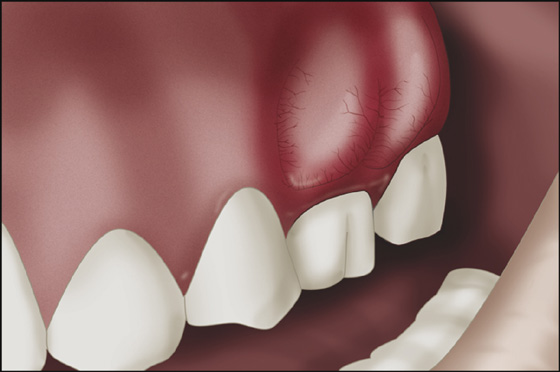
Figure 45-4 Abscess adjacent to primary tooth.
 Instruct the patient to apply warm compresses to the affected area and seek follow-up care from a dentist within 24 hours. Definitive therapy is root canal treatment or extraction.
Instruct the patient to apply warm compresses to the affected area and seek follow-up care from a dentist within 24 hours. Definitive therapy is root canal treatment or extraction.
 When drug-seeking behavior is suspected, limit narcotic prescriptions, and assist the patient by ensuring that early dental consultation is obtained.
When drug-seeking behavior is suspected, limit narcotic prescriptions, and assist the patient by ensuring that early dental consultation is obtained.
What Not To Do:
 Do not obtain radiographs for an uncomplicated abscess.
Do not obtain radiographs for an uncomplicated abscess.
 Do not insert an obstructing pack (i.e., cotton soaked with oil of cloves) into a tooth cavity when an abscess or cellulitis is present.
Do not insert an obstructing pack (i.e., cotton soaked with oil of cloves) into a tooth cavity when an abscess or cellulitis is present.
 Do not prescribe aspirin if it is possible that a tooth will need to be extracted.
Do not prescribe aspirin if it is possible that a tooth will need to be extracted.
A periapical abscess originates in the dental pulp, usually secondary to dental caries that erode the protective layers of the tooth (enamel, dentin) and allow bacteria to invade the pulp, producing a pulpitis. A severely inflamed pulp (pulpitis) will eventually necrose, causing apical periodontitis, which is inflammation around the apex of the tooth. Apical abscess is a localized, purulent form of apical periodontitis. Cellulitis may follow apical periodontitis or abscess if the infection spreads into the surrounding tissues (see Figure 45-4). This is the most common dental abscess in children.
Dental pain may be referred to the ear, temple, eye, neck, or other teeth. Conversely, what appears to be dental pain may, in fact, be caused by overlying maxillary sinusitis or otitis.
Diabetes, immune deficiency diseases, and valvular heart disease increase the risk for complications from bacteremia. Local extension of infection can lead to retropharyngeal abscess, Ludwig cellulitis, cavernous sinus thrombosis, osteomyelitis, mediastinitis, and pulmonary abscess, which are all serious complications requiring immediate consultation with an appropriate specialist.
An acute periodontal (as opposed to periapical) abscess, involves the supporting structures of the teeth (periodontal ligaments, alveolar bone), and causes localized, painful, fluctuant swelling of the gingiva, either between the teeth or laterally, and is associated with vital teeth that are not usually sensitive to percussion. This condition is found in patients with chronic periodontal disease and is the most common dental abscess in adults. It may also occur in patients (including children) who have a foreign object lodged in the gingiva. The involved tooth may be tender to percussion and show increased mobility. Treatment consists of local infiltrative anesthesia and drainage by subgingival curettage. In severe cases or cases in which there is fever, prescribe doxycycline, 100 mg bid for 10 days. Also, instruct the patient to rinse his mouth with warm salt water and consult a dentist for further treatment. Severe periodontitis in a young patient should raise the possibility of an underlying immune disorder.

Full access? Get Clinical Tree


