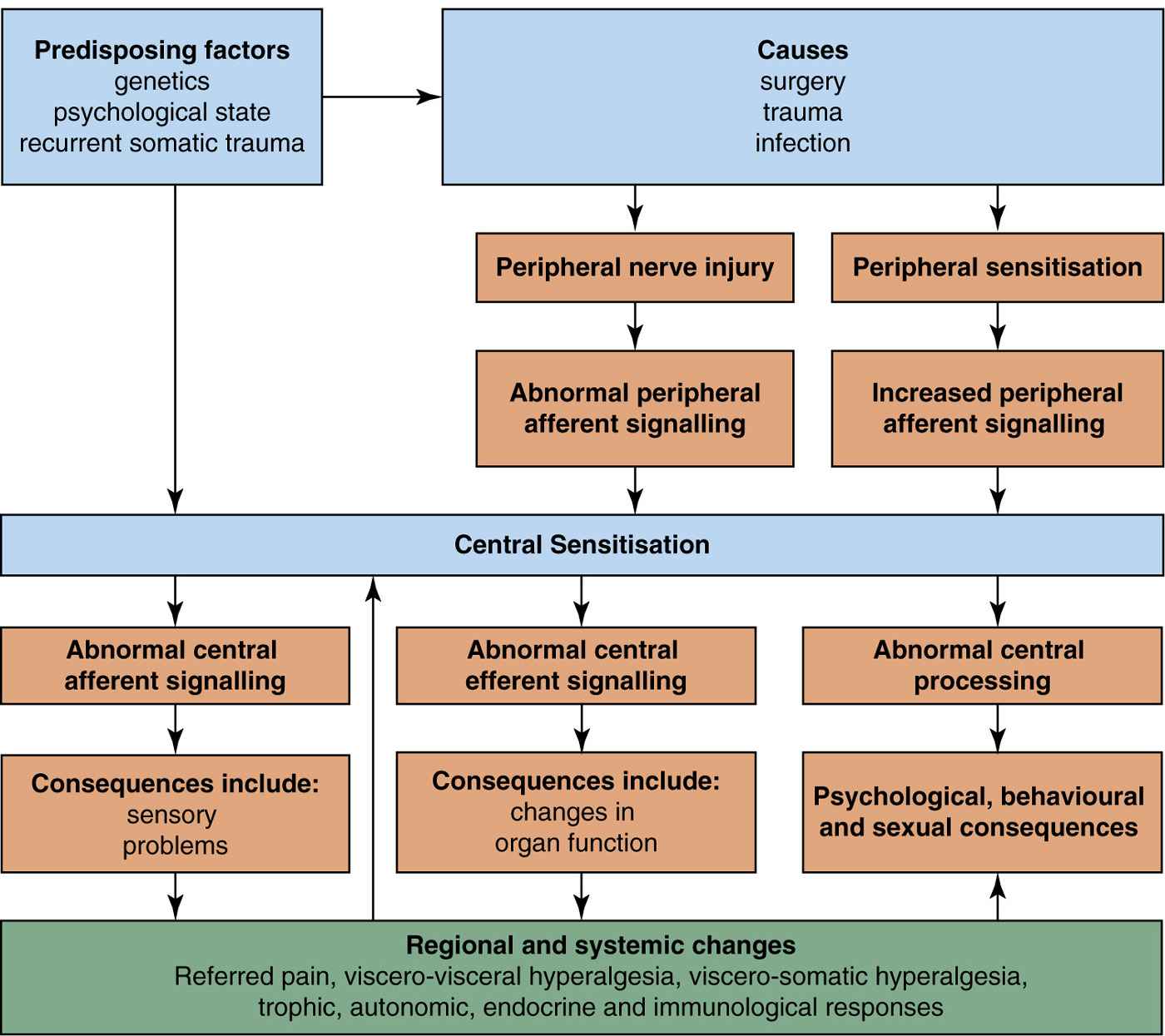
A newer and different representation of the classification has been developed by the EAU in order to aid both an academic and clinical understanding of this patient group (Fig. 1)[4]. This covers the predisposing factors, causes, central and peripheral mechanisms. Some detail can be added to each of the boxes but it is also understood that there remains a significant amount to be elucidated.
It is not prescriptive about a cause but does suggest predisposing factors. The basic science elements have a significant amount of understanding but gaps remain. This model allows alterations in organ function that may have a central component, altered sensory perception, changes in psychological, behavioural, and sexual function. This is true for all the pelvic pain syndromes and the balance and complexion of presentation will vary from patient to patient which again this model allows.
FUTURE DEVELOPMENTS
Along with this strand of work there has been a significant amount of parallel developments and potential avenues for further exploration.
Guidelines and pathways have become very popular over recent years in many countries. The European Association of Urology[4] has taken this to heart and the chronic pelvic pain guidelines have been well received and frequently downloaded by a wide range of specialities. They are updated very regularly and have open access for download. There are other published guidance documents from organisations such as: American Urological Association[6], American committee of obstetrics and gynaecology[1], Royal College of Obstetrics and Gynaecology[8,9], British Society for the Study of Vulval Disease (BSSVD)[10], International Consultation on Incontinence[5], this is not an exhaustive list. Often the guidance is aimed at relatively specific groups such as endometriosis, vulvodynia, bladder pain syndrome but some are broader in direction. More recently the British Pain Society[11] in conjunction with the map of medicine have developed a patient pathway which is evidence based, reference graded and externally reviewed with the aim of supporting primary care physicians manage this patient population and a second part for secondary care. The committee that developed the pathway included patients and was truly multiprofessional.
Education in pain management is poorly taught across many disciplines in a general sense [3,12,14]. There has been debate as to what and how to train health care workers with regard to pelvic and abdominal pain. This includes what and at what depth but also who to develop and how to make the teams managing these patients most effective. The clarification of terminology and growing understanding of management strategies should help develop this strand of work.




Full access? Get Clinical Tree


