![]() To provide emergent airway access only when a safer, less invasive airway cannot be established or is contraindicated
To provide emergent airway access only when a safer, less invasive airway cannot be established or is contraindicated
![]() For children younger than 12 years, needle cricothyroidotomy is the surgical airway of choice
For children younger than 12 years, needle cricothyroidotomy is the surgical airway of choice
CONTRAINDICATIONS
![]() Absolute
Absolute
![]() An oral or nasal airway can be established
An oral or nasal airway can be established
![]() Significant injury or fracture of the cricoid cartilage or larynx (tracheostomy is the procedure of choice)
Significant injury or fracture of the cricoid cartilage or larynx (tracheostomy is the procedure of choice)
![]() Tracheal fracture or transection
Tracheal fracture or transection
![]() Obstruction below the cricothyroid membrane
Obstruction below the cricothyroid membrane
![]() Patients younger than 12 years (needle cricothyroidotomy is the procedure of choice for this age-group)
Patients younger than 12 years (needle cricothyroidotomy is the procedure of choice for this age-group)
![]() Relative
Relative
![]() Neck mass, swelling, or cellulitis
Neck mass, swelling, or cellulitis
![]() Neck hematoma
Neck hematoma
![]() Coagulopathy
Coagulopathy
LANDMARKS
![]() The cricothyroid membrane—an elastic membrane located anteriorly and midline in the neck, measuring 9 mm longitudinally and 30 mm transversely. Bordered superiorly by the thyroid cartilage (“Adam’s apple”) and inferiorly by the cricoid cartilage.
The cricothyroid membrane—an elastic membrane located anteriorly and midline in the neck, measuring 9 mm longitudinally and 30 mm transversely. Bordered superiorly by the thyroid cartilage (“Adam’s apple”) and inferiorly by the cricoid cartilage.
![]() In children, the larynx is positioned more superiorly than in adults and is relatively smaller in size (FIGURES 6.1 and 6.2)
In children, the larynx is positioned more superiorly than in adults and is relatively smaller in size (FIGURES 6.1 and 6.2)
STANDARD CRICOTHYROIDOTOMY
![]() Supplies
Supplies
![]() Antiseptic solution, drapes, towel clips
Antiseptic solution, drapes, towel clips
![]() Lidocaine with epinephrine
Lidocaine with epinephrine
![]() No. 11 blade scalpel with handle
No. 11 blade scalpel with handle
![]() Tracheal hook
Tracheal hook
![]() Trousseau dilator
Trousseau dilator
![]() Tracheostomy tube
Tracheostomy tube
![]() Neck tie or sutures
Neck tie or sutures
![]() Technique
Technique
![]() Preparation
Preparation
![]() Hyperextend the neck to more readily identify landmarks, unless the patient has a known or suspected cervical spine injury
Hyperextend the neck to more readily identify landmarks, unless the patient has a known or suspected cervical spine injury
![]() Preoxygenate the patient by bag-mask ventilation
Preoxygenate the patient by bag-mask ventilation
![]() Test the integrity of the balloon on the tracheostomy tube by injecting with 10 mL of air
Test the integrity of the balloon on the tracheostomy tube by injecting with 10 mL of air
![]() If time permits, apply appropriate antiseptic solution and drape the area with sterile towels
If time permits, apply appropriate antiseptic solution and drape the area with sterile towels
![]() If time permits and patient is conscious or responding to pain, infiltrate the skin of anterior neck with 1% lidocaine solution with epinephrine
If time permits and patient is conscious or responding to pain, infiltrate the skin of anterior neck with 1% lidocaine solution with epinephrine
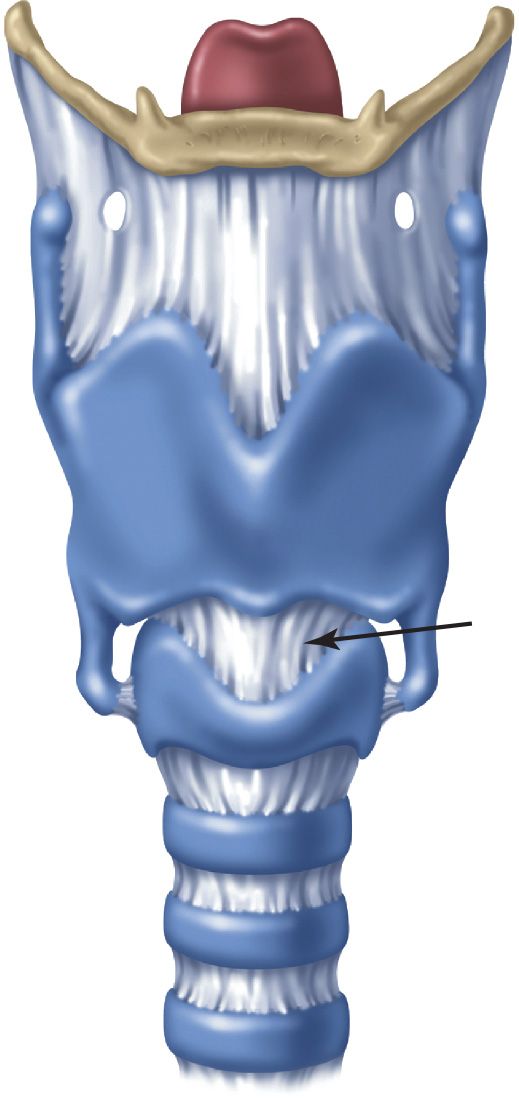
FIGURE 6.1 Anatomy of the larynx. The cricothyroid membrane (arrow) is bordered above by the thyroid cartilage and below by the cricoid cartilage. (From Walls RM, Murphy MF. Manual of Emergency Airway Management. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2012:162, with permission.)
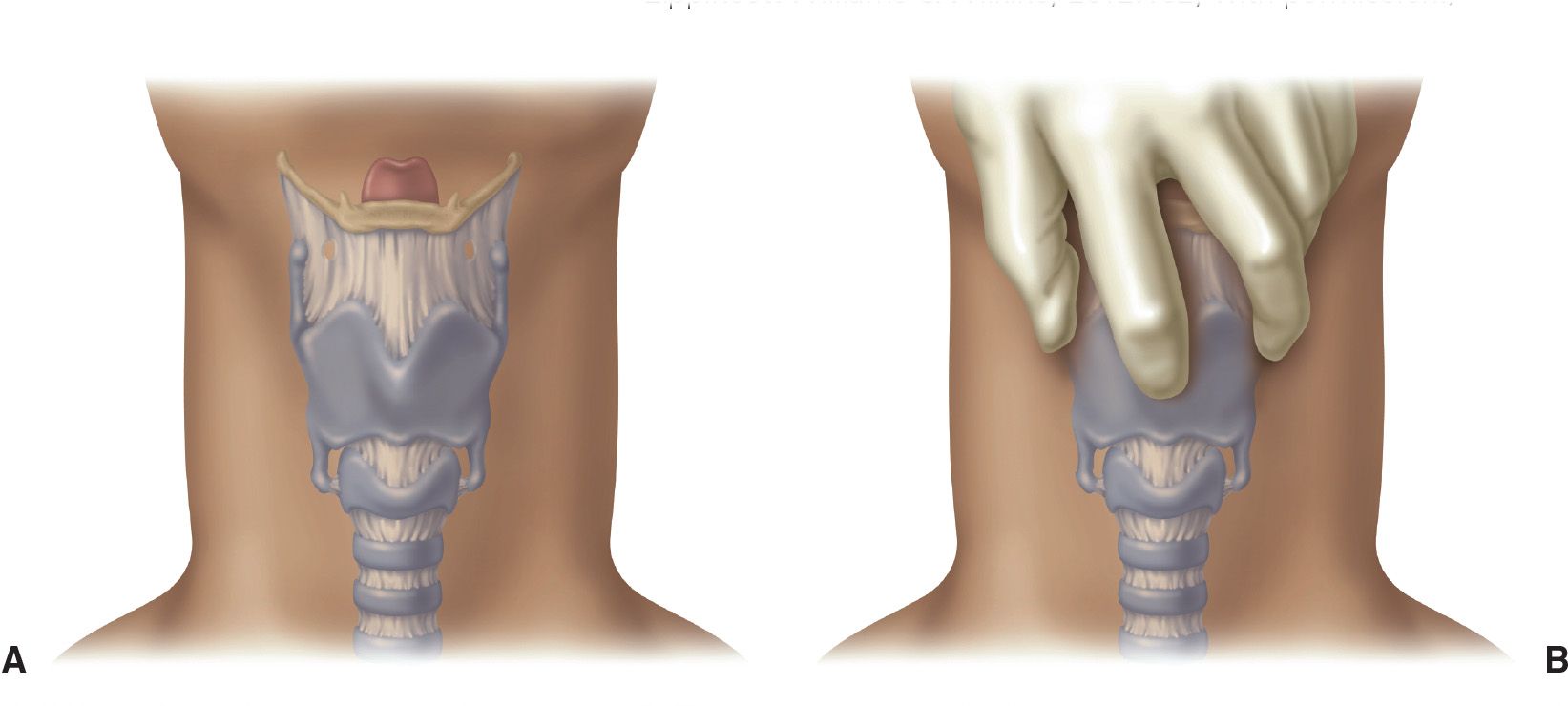
FIGURE 6.2 A: Surface anatomy of the airway. B: The thumb and middle finger immobilize the superior cornua of the larynx; the index finger palpates the cricothyroid membrane. (From Walls RM, Murphy MF. Manual of Emergency Airway Management. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2012:163, with permission.)
![]() General Basic Steps
General Basic Steps
![]() Identify the landmarks
Identify the landmarks
![]() Stabilize the larynx
Stabilize the larynx
![]() Incise the skin
Incise the skin
![]() Reidentify the cricothyroid membrane
Reidentify the cricothyroid membrane
![]() Incise the cricothyroid membrane
Incise the cricothyroid membrane
![]() Insert the tracheal hook
Insert the tracheal hook
![]() Insert the trousseau dilator
Insert the trousseau dilator
![]() Insert the tracheostomy tube
Insert the tracheostomy tube
![]() Inflate the cuff and confirm tube position
Inflate the cuff and confirm tube position
![]() Secure the tracheostomy tube
Secure the tracheostomy tube
![]() Identify the Landmarks (See Earlier “Landmarks” Section)
Identify the Landmarks (See Earlier “Landmarks” Section)
![]() Stabilize the Larynx
Stabilize the Larynx
![]() Grasp both sides of the thyroid cartilage with the thumb and middle finger using the nondominant hand
Grasp both sides of the thyroid cartilage with the thumb and middle finger using the nondominant hand
![]() Palpate the depression over the cricothyroid membrane with the index finger
Palpate the depression over the cricothyroid membrane with the index finger
![]() Control the larynx throughout the procedure by stabilizing it in this manner and reidentify the cricothyroid membrane at any time during the procedure
Control the larynx throughout the procedure by stabilizing it in this manner and reidentify the cricothyroid membrane at any time during the procedure
![]() Incise the Skin
Incise the Skin
![]() Using a no. 11 scalpel blade in the dominant hand, make a vertical midline incision through the skin and subcutaneous tissue approximately 2 to 3 cm in length
Using a no. 11 scalpel blade in the dominant hand, make a vertical midline incision through the skin and subcutaneous tissue approximately 2 to 3 cm in length
![]() Care should be taken to extend the incision down to but not through any of the deep structures of the neck
Care should be taken to extend the incision down to but not through any of the deep structures of the neck
![]() Reidentify the Cricothyroid Membrane
Reidentify the Cricothyroid Membrane
![]() Using the index finger of the nondominant hand, reidentify the cricothyroid membrane while maintaining immobilization of the larynx with the thumb and middle finger
Using the index finger of the nondominant hand, reidentify the cricothyroid membrane while maintaining immobilization of the larynx with the thumb and middle finger
![]() If the cricothyroid membrane cannot be palpated, extend the initial incision superiorly and inferiorly and try to palpate again
If the cricothyroid membrane cannot be palpated, extend the initial incision superiorly and inferiorly and try to palpate again
![]() Incise the Cricothyroid Membrane
Incise the Cricothyroid Membrane
![]() Using the stabilizing index finger as a guide, incise the cricothyroid membrane at least 1 cm in length in the horizontal direction
Using the stabilizing index finger as a guide, incise the cricothyroid membrane at least 1 cm in length in the horizontal direction
![]() Note that the skin incision is vertical and the incision through the membrane is horizontal
Note that the skin incision is vertical and the incision through the membrane is horizontal
![]() Place the index finger into the stoma temporarily while exchanging the scalpel for the tracheal hook
Place the index finger into the stoma temporarily while exchanging the scalpel for the tracheal hook
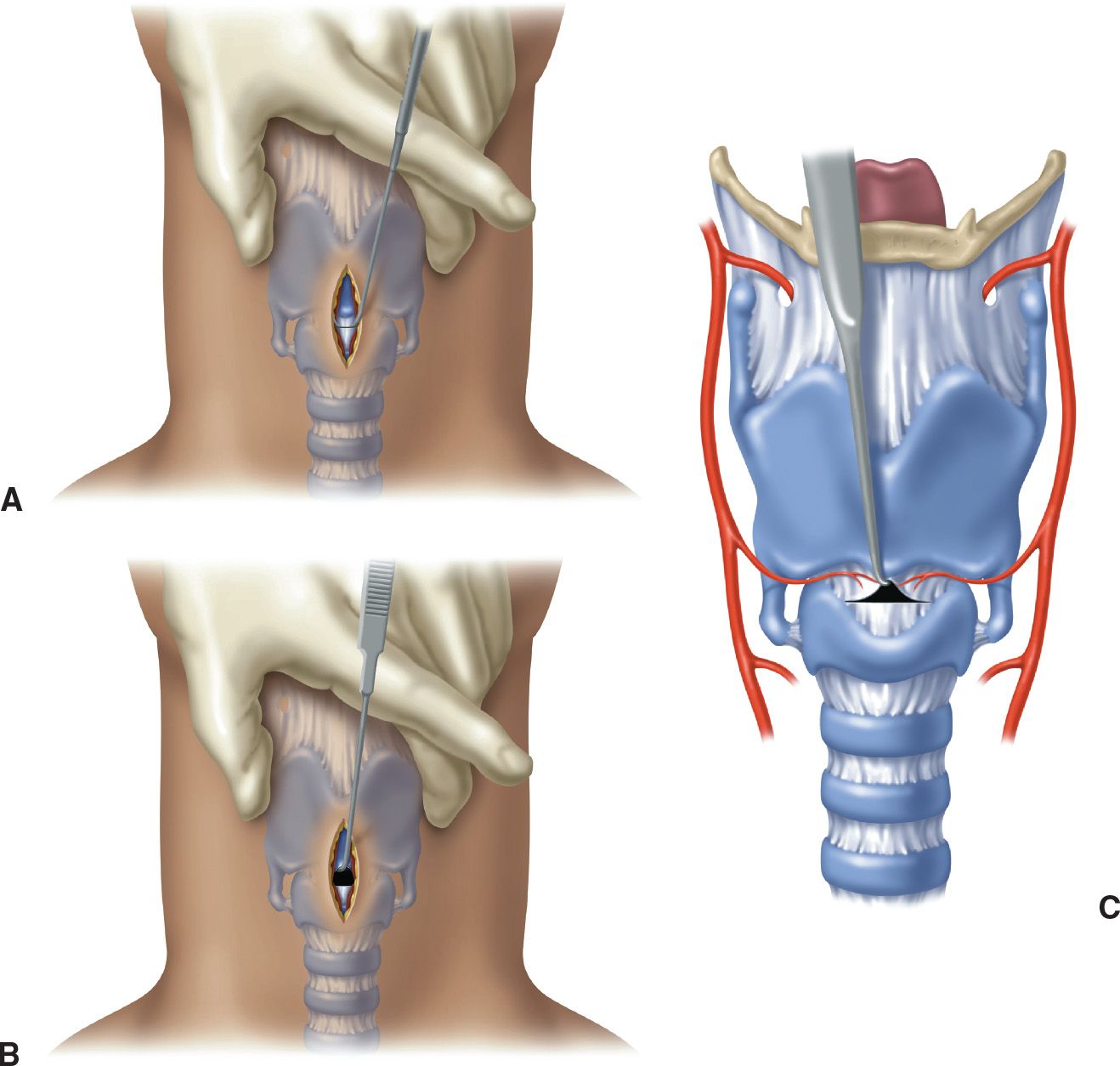
FIGURE 6.3 A: The tracheal hook is oriented transversely during insertion. B and C: After insertion, cephalad traction is applied to the inferior margin of the thyroid cartilage. (From Walls RM, Murphy MF. Manual of Emergency Airway Management. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2012:166, with permission.)

Full access? Get Clinical Tree


