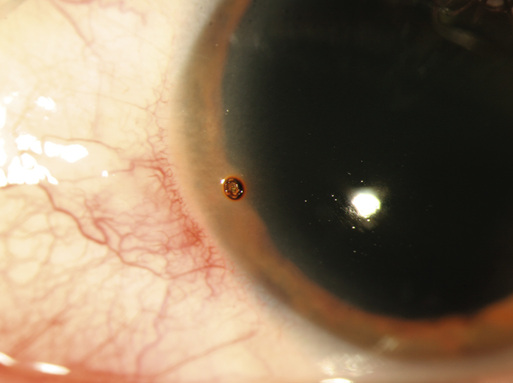
Neda Nikpor, James T. Banta A corneal surface defect occurs when the corneal epithelium is interrupted. Direct trauma from foreign objects (e.g., fingers, tree branches, makeup applicators) typically causes these injuries. Airbags from motor vehicle accidents are another common source of injury. Contact lens wearers are particularly susceptible to corneal problems because prolonged use of lenses can result in injury and corneal epithelial breaks.1 In most cases, the patient can recall a specific moment when trauma occurred. Corneal surface foreign bodies are particularly common in workers who spend time around small particles or dust or who grind metal, such as construction workers, mechanics and landscapers (Fig. 74-1).2 Chemicals, either splashed or inadvertently placed in the eye, can also cause surface defects. These injuries are almost universally preventable with the appropriate type of eye protection. Corneal surface defects must be distinguished from other serious conditions, most notably corneal inflammatory conditions, lacerations, and infections. Full-thickness lacerations can occur with ocular trauma and sometimes appear clinically similar to epithelial defects. Infectious keratitis, or corneal ulcers, are common in contact lens users. An ulcer is an epithelial defect with an infiltrate, or white area in the cornea. Other common conditions with similar presentations include herpetic keratitis, staphylococcal marginal disease, and phlyctenulosis, the last two frequently manifesting as peripheral corneal opacities with associated epithelial defects. An abrasion of the corneal epithelium may be caused by chemical or mechanical debridement resulting from trauma, chemicals, or ultraviolet radiation exposure. Corneal erosions occur if an abrasion disrupts Bowman’s layer. Decreased evaporation during sleep results in the formation of a fluid layer above the incompletely healed Bowman’s layer and below the epithelium. This can lead to repeated sloughing of the overlying epithelium when the patient awakens and opens the lid, given the relative lack of epithelial adherence. Epithelial defects, whether abrasions or erosions, may allow bacterial, viral, or fungal organisms to invade the corneal stroma, resulting in an ulcer. Sterile corneal ulcers may also occur. The most common symptom of a corneal abrasion or foreign body is sudden onset of severe eye pain in the affected eye. This pain typically resolves after application of a topical anesthetic eye drop.3 Some patients may report a foreign body sensation instead of severe pain. Other symptoms include blurred vision, redness, tearing, light sensitivity, eyelid swelling, and blepharospasm.4 On examination, vision may be limited if the epithelial defect or foreign body falls within the visual axis. The pupils should react normally to light, and eye pressure is typically not affected. The eyelids may appear swollen in the affected eye, and the conjunctiva is typically injected. The cornea may have some mild haze but should not be focally opacified. If there is a significant corneal opacity, an alternative diagnosis such as infectious keratitis should be considered. A foreign body may be visible on the corneal or conjunctival surface. The anterior chamber should have normal depth, and the iris should have a normal, round appearance. Presence of a hypopyon (inflammatory debris layering in the inferior portion of the anterior chamber) suggests a more serious diagnosis, and immediate referral should be made to an ophthalmologist. If the anterior chamber appears flattened or the pupil is peaked or irregular, this suggests a penetrating injury, and immediate referral should be made to an ophthalmologist. Use of topical fluorescein dye can assist in the diagnosis of a corneal surface defect. One drop of fluorescein can be applied and viewed under a cobalt blue light or Wood lamp. A corneal abrasion should appear as a bright green area, often polygonal (Fig. 74-2). Linear, vertically oriented epithelial defects are typically caused by subtarsal (trapped under the upper eyelid) foreign bodies and should prompt eversion of the upper eyelids to check for foreign material. Fluorescein staining of true surface defects should not change with the patient’s blinking. If the defect appears to have a branching or dendritic pattern, a herpetic cause should be entertained. An irregular iris and a shallow anterior chamber associated with an area of fluorescein staining raise the specter of a full-thickness corneal laceration and should prompt emergent ophthalmology referral. Diagnostics Corneal Surface Defects and Foreign Bodies
Corneal Surface Defects and Ocular Surface Foreign Bodies
Definition and Epidemiology
Pathophysiology
Clinical Presentation
Physical Examination
Diagnostics
Corneal Surface Defects and Ocular Surface Foreign Bodies
Chapter 74