Chapter 23 Cor Pulmonale
2 What are the subtypes of cor pulmonale?
Cor pulmonale can be acute or chronic.
 In acute cor pulmonale the afterload to the right ventricle can rise in a matter of minutes (e.g., massive pulmonary embolism) giving very little room for compensation. The result will be acute right ventricular dilatation and failure, its severity depending primarily on the degree of acute PA hypertension.
In acute cor pulmonale the afterload to the right ventricle can rise in a matter of minutes (e.g., massive pulmonary embolism) giving very little room for compensation. The result will be acute right ventricular dilatation and failure, its severity depending primarily on the degree of acute PA hypertension.

3 What is the pathophysiology of right ventricular failure?
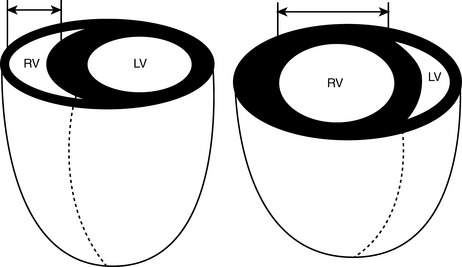
Under normal conditions, the pulmonary circulation is a low-resistance circuit, and the right ventricle generates the same stroke volume as the left ventricle with end-systolic pressures that are just 20% to 25% of those in the left ventricle. The low pressure within the thin free wall of the right ventricle also allows myocardial perfusion to occur both in systole and in diastole. Because of its structure, similar to that of veins rather than arteries, the right ventricle accommodates well additional volume but not higher pressure. When pressure overload occurs acutely, the right ventricle can only dilate and, if the pressure is sufficiently elevated, fail. Chronically, in response to increased systolic workload the free wall of the right ventricle hypertrophies and becomes similar to the left ventricle. Laplace’s law helps explaining the evolution from hypertrophy to dilatation and failure (Fig. 23-1): In a thin-wall chamber, an increase in intraluminal pressure increases wall stress unless thickness increases or the internal radius decreases. As the right ventricle hypertrophies, myocardial perfusion becomes limited to diastole, making its myocardium more susceptible to ischemia, and thus leading to dilatation and failure.
4 What are the causes of cor pulmonale?
Any process that results in pulmonary hypertension can cause cor pulmonale. Pulmonary hypertension is defined as mean PA pressures > 20 mm Hg at rest or > 30 mm Hg with exercise. The most frequent cause of pulmonary hypertension and cor pulmonale is COPD, due to chronic hypoxemia. In COPD the degree of hypertension is generally moderate, and oxygen supplementation may be effective in relieving some of the pressure load to the right ventricle and delaying failure. Additional causes of cor pulmonale include chronic pulmonary thromboembolic disease, left-sided cardiac abnormalities, untreated obstructive sleep apnea (OSA), interstitial lung diseases, and primary pulmonary hypertension. A comprehensive classification of the diseases of the lung associated with PA hypertension and cor pulmonale is shown in Table 23-1.
Table 23-1 Classification of cor pulmonale according to causative factor
| Category | Example |
|---|---|
| Diseases affecting the air passages of the lung and alveoli | COPD Cystic fibrosis Infiltrative or granulomatous defects Idiopathic pulmonary fibrosis Sarcoidosis Pneumoconiosis Scleroderma Mixed connective tissue disease Systemic lupus erythematosus Rheumatoid arthritis Polymyositis Eosinophilic granulomatosis Radiation Malignant infiltration |
| Diseases affecting thoracic cage movement | Kyphoscoliosis Thoracoplasty Neuromuscular weakness Sleep apnea syndrome Idiopathic hypoventilation |
| Diseases affecting the pulmonary vasculature | Primary disease of the arterial wall Primary pulmonary hypertension Pulmonary arteritis Toxin-induced pulmonary hypertension Chronic liver disease Peripheral pulmonary stenosis |
| Thrombotic disorders | Sickle cell diseases Pulmonary microthrombi |
| Embolic disorders | Thromboembolism Tumor embolism Other embolic processes (amniotic fluid, air, fat) Schistosomiasis and other parasitic infections |
| Pressure on PAs | Mediastinal tumors Aneurysms Granulomata Fibrosis |
Modified from Rubin LJ, ed: Pulmonary Heart Disease. Boston, 1984, Martinus Nijhoff, p 4.
7 What are the signs and symptoms of cor pulmonale?
Symptoms of cor pulmonale include the following:






Signs of cor pulmonale include the following:






9 What are the electrocardiographic (ECG) findings associated with right ventricular hypertrophy?
 Right axis deviation: QRS negative in lead I, positive in aVR
Right axis deviation: QRS negative in lead I, positive in aVR
 Tall R waves in the right precordial leads, deep S waves in the left precordial leads
Tall R waves in the right precordial leads, deep S waves in the left precordial leads
 Right atrial enlargement: P pulmonale, large P wave, in II and V1
Right atrial enlargement: P pulmonale, large P wave, in II and V1
 ST-segment changes in the opposite direction of the QRS (i.e., wide QRS-ST angle)
ST-segment changes in the opposite direction of the QRS (i.e., wide QRS-ST angle)
 Right bundle branch block: wide QRS (> 1.12 seconds); RSR′ in V1 and V2
Right bundle branch block: wide QRS (> 1.12 seconds); RSR′ in V1 and V2

Full access? Get Clinical Tree


