Continuous Sciatic Nerve Blocks
Maria Matuszczak
Didier Sciard
A. Parasacral Approach
Table 60-1. Maximum Initial Bolus Volume of Ropivacaine 0.2%—Parasacral Approach | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
 Figure 60-1. Parasacral catheter placement. |
The needle is introduced perpendicular to the skin or 30° in the cranial direction.
At this level the sciatic nerve is close to the internal iliac vessels (sciatic vascular trunk).
If there is bone contact, the needle needs to be inserted more caudally on the line between the posterior superior iliac spine and the ischial tuberosity.
A stimulating catheter can be used in older children.
Suggested Readings
Dadure C, Capdevila X. Continuous peripheral nerve blocks in children. Best Pract Res Clin Anaesthesiol 2005;19(2):309–321.
Dadure C, Pirat Ph, Raux O, et al. Perioperative continuous peripheral nerve blocks with disposable infusion pumps in children: a prospective descriptive study. Anesth Analg 2003;97:687–690.
Dalens B. Regional anesthesia in infants, children, and adolescents. Baltimore: Williams & Wilkins, 1995.
Ivani G, Mossetti V. Continuous peripheral nerve blocks. Paediatr Anaesth 2005;15:87–90.
B. Anterior Approach
through the greater trochanter. A perpendicular line is drawn at the junction of the medial third and the lateral two-thirds of these lines. The intersection of the perpendicular line and the line passing through the greater trochanter presents the site of needle insertion. In an appropriately anesthetized/sedated child, the insulated needle, connected to a nerve stimulator (1.5 mA, 2 Hz, 0.1 ms) is introduced perpendicular to the skin. Within 3 to 11 cm, a sciatic nerve stimulation is elicited. With an appropriate muscle response still present at a current of 0.5 mA and after negative aspiration for blood the appropriate amount of local anesthetic solution is slowly injected. Maintaining the introducer needle in the same position, the catheter is threaded 2 cm beyond the needle tip. The introducer needle is removed and the catheter is secured in place with benzoin and a transparent adhesive dressing.
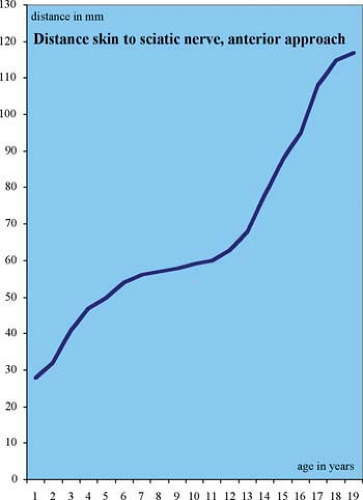 Figure 60-2. Distance skin to sciatic nerve, anterior approach distance. |
Table 60-2. Maximum Initial Bolus Volume of Ropivacaine 0.2%—Anterior Approach | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
A femoral nerve stimulation may be elicited within a depth of 1 to 4 cm.
The needle has to be withdrawn very carefully in order not to displace the catheter.
If the femur is contacted the needle has to be introduced more medially.
To the authors’ knowledge this approach was not yet used for continuous infusion in smaller children. The youngest patient with continuous infusion was 15 years old (43 kg).
A stimulating catheter can be used in older children.
Suggested Readings
Beck GP. Anterior approach to sciatic nerve block. Anesthesiology 1963;24:222–224.
Chelly JE, Greger J, Howard G. Simple interior approach for sciatic blockade. Reg Anesth 1997;22:114.
Dadure C, Capdevila X. Continuous peripheral nerve blocks in children. Best Pract Res Clin Anaesthesiol 2005;19(2):309–321.
Dadure C, Pirat Ph, Raux O, et al. Perioperative continuous peripheral nerve blocks with disposable infusion pumps in children: a prospective descriptive study. Anesth Analg 2003;97:687–690.
Dalens B. Regional anesthesia in infants, children, and adolescents. Baltimore: Williams & Wilkins, 1995.
Ivani G, Mossetti V. Continuous peripheral nerve blocks. Paediatr Anaesth 2005;15:87–90.
Raj PP, Parks RI, Watson TD, et al. A new single-position supine approach to sciatic-femoral nerve block. Anesth Analg 1975; 54:489–493.
C. Subgluteal Approach
Related posts:



Full access? Get Clinical Tree


