Continuous Lumbar Plexus Blocks
Maria Matuszczak
Didier Sciard
A. Psoas Compartment Approach
position, the catheter is threaded 2 cm beyond the needle tip. The introducer needle is removed and the catheter is secured in place with benzoin and a transparent adhesive dressing. Blood pressure has to be monitored because of a possible epidural or subarachnoid injection. The absence of epidural spread is assessed by the presence of an adequate reaction to pinprick of the opposite leg after emergence.
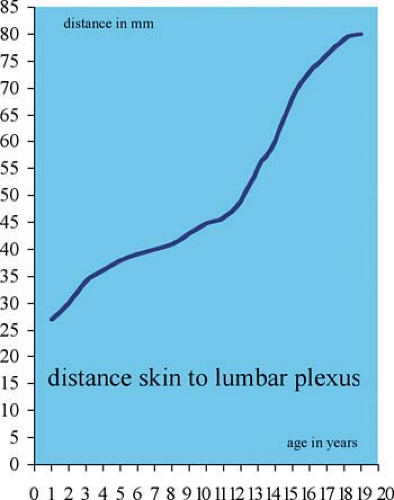 Figure 59-1. Distance skin to lumbar plexus. |
This block should only be performed by an anesthesiologist trained in pediatric regional techniques.
The technique described above is Winnie’s approach; we do not use Chayen’s approach because of a higher incidence of epidural spread reported in the literature.
The shortest needle that can easily reach the plexus has to be used because of the potential risk of visceral organ (kidney) puncture.
Ultrasound guidance can help to determine the depth of the lumbar plexus.
Peritoneal or visceral infection, trauma to the lumbar spine, lumbar vertebral deformities, and coagulopathy are contraindications for this block.
A slow injection (1 mL/10 seconds) of the local anesthetic is advised.
The absence of epidural spread is assessed by the presence of an adequate reaction to a pinprick of the opposite leg after emergence from anesthesia.
A stimulating catheter can be used in older children.
Table 59-1. Maximum Initial Bolus Volume of Ropivacaine 0.2%—Psoas Compartment Approach | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
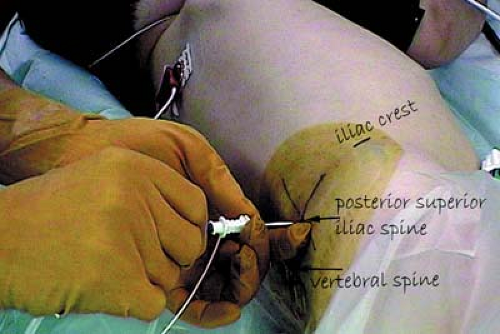 Figure 59-2. Lumbar plexus landmarks. |
 Figure 59-3. Lumbar plexus catheter placement. |
Suggested Readings
Chayen D, Nathan H, Chayen M. The psoas compartment block. Anesthesiology 1976;45:95–99.
Dadure C, Capdevila X. Continuous peripheral nerve blocks in children. Best Pract Res Clin Anaesthesiol 2005;19(2):309–321.
Dadure C, Pirat Ph, Raux O, et al. Perioperative continuous peripheral nerve blocks with disposable infusion pumps in children: A prospective descriptive study. Anesth Analg 2003;97:687–690.
Dadure C, Raux O, Gaudard P, et al. Continuous psoas compartment blocks after major orthopedic surgery in children: a prospective computed tomographic scan and clinical studies. Anesth Analg 2004;98(3):623–628.
Related posts:



Full access? Get Clinical Tree


