Continuous Lumbar Plexus Blocks
A. Continuous Lumbar Plexus Block
Jacques E. Chelly
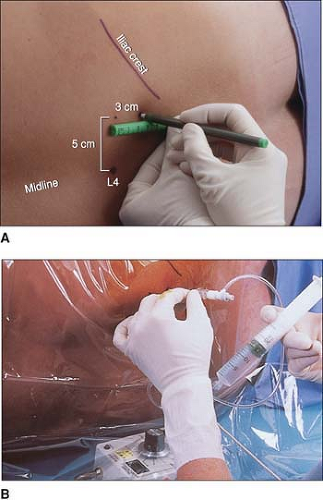 Figure 28-1. The lumbar plexus is identified and the needle is advanced. |
When combined with a sciatic nerve block, this block may provide surgical anesthesia to the lower extremity.
Epidural spread and/or injections may result in a bilateral block.
A loss-of-resistance technique can be used, especially when the block is performed for postoperative analgesia.
A more medial approach has been described (3.5 cm from the spinous process).
Continuous lumbar plexus blocks should not be performed in anticoagulated patients, because of the risk of retroperitoneal hematoma.
Suggested Readings
Awad IT, Duggan EM. Posterior lumbar plexus block: Anatomy, approaches, and techniques. Reg Anesth Pain Med 2005;30:143–149.
Capdevila X, Coimbra C, Choquet O. Approaches to the lumbar plexus: success, risks and outcome. Reg Anesth Pain Med 2005;35:150–162.
Capdevila X, Macaire P, Dadure C, et al. Continuous psoas compartment block for postoperative analgesia after total hip arthroplasty: new landmarks, technical guidelines, and clinical evaluation. Anesth Analg 2002;94:1606–1613.
Chudinov A, Berkenstadt H, Salai M, et al. Continuous psoas compartment block for anesthesia and perioperative analgesia in patients with hip fractures. Reg Anesth Pain Med 1999;4:563–568.
Klein S, D’Ecole F, Greengrass R, et al. Enoxaparin associated with psoas hematoma and lumbar plexopathy after lumbar plexus block. Anesthesiology 1997;87:1576–1579.
Mansour NY, Bennetts FE. An observational study of combined continuous lumbar plexus and single-shot sciatic nerve blocks for post-knee surgery analgesia. Reg Anesth 1996;21:287–291.
Schultz P, Anker-Moller E, Dahl JB, et al. Postoperative pain treatment after open knee surgery: continuous lumbar plexus block with bupivacaine versus epidural morphine. Reg Anesth 1991;16:34–37.
White IW, Chappell WA. Anaesthesia for surgical correction of fractured femoral neck: a comparison of three techniques. Anaesthesia 1980;35:1107–1110.






