Continuous Brachial Plexus Blocks
Continuous Brachial Plexus Blocks
Maria Matuszczak
Didier Sciard
A. Interscalene Approach
 Patient Position:
Patient Position: Supine, with the head slightly turned away from the side where the block is performed, and the arm extended along the side of the body.
 Indications:
Indications: Anesthesia and postoperative analgesia for shoulder surgery.
 Needle Size and Catheter:
Needle Size and Catheter: 18-gauge, 38-mm insulated introducer Tuohy needle and a 20- or 21-gauge catheter.
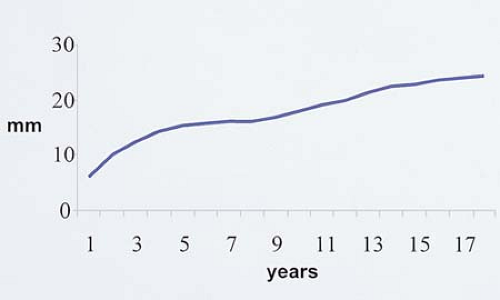
 Skin–Nerve Distance:
Skin–Nerve Distance: 0.6 cm (5 mm) at the age of 1 year, 2.5 cm (5 mm) at the age of 18 years
(Fig. 57-1).
 Anatomic Landmarks:
Anatomic Landmarks: The lateral border of the sternocleidomastoid muscle is identified and marked. Posteriorly, the groove between the anterior and the middle scalene muscle is identified. Next, a line is drawn at the level of the cricoid cartilage. At the intersection of these two lines, the brachial plexus will be found in the interscalene groove.
 Approach and Technique:
Approach and Technique: The insertion point should be high in the interscalene groove. In an appropriately anesthetized/sedated child, the insulated introducer Tuohy needle, connected to a nerve stimulator (1.5 mA, 2 Hz, 0.1 ms), is positioned parallel to the neck, close to the external jugular vein and directed anteriorly to the interscalene groove. After appropriate positioning of the needle to maintain the muscle response with a current of 0.5 mA, the local anesthetic solution is slowly injected after negative aspiration for blood. Maintaining the insulated introducer needle in the same position, the catheter is threaded 2 cm beyond the needle tip. The Tuohy needle is removed, and the catheter is
secured in place with Steri-Strip (3M, St. Paul, MN) and covered with a transparent dressing
(Fig. 57-2).
 Tips
Tips
The site of introduction of the needle is often lateral and posterior to the jugular vein.
A stimulation of the musculocutaneous nerve or the median nerve is preferred to a stimulation of the axillary nerve (deltoid contraction).
The roots C8 and T1 (ulnar and median nerves) are partially blocked or not blocked with this approach.
If a trapezius contraction is elicited, indicating a stimulation of the dorsal scapular root, the needle is too posterior and should be redirected more anteriorly.
If a diaphragm contraction is elicited, indicating a stimulation of the phrenic nerve, the needle is too anterior and should be redirected more posteriorly.
A needle position parallel to the plexus sheath allows a better introduction of the catheter.
Only gold members can continue reading.
Log In or
Register to continue
Related

Full access? Get Clinical Tree