Chapter 3 Complications of Cranial Nerve Stimulation
 Appropriate Accreditation Council for Graduate Medical Education mentored subspecialty training in interventional pain management is vital to ensure patient-centered care.
Appropriate Accreditation Council for Graduate Medical Education mentored subspecialty training in interventional pain management is vital to ensure patient-centered care.




Introduction
Cranial nerve stimulation strategies have been used to treat a variety of diverse conditions that sometimes prove to be unresponsive to conservative medical therapies. These range from depression to seizure to congestive heart failure.1–3 More specifically, some other indications include atypical facial pain, terminal branch neuralgias, a variety of headache disorders (i.e., cluster, migraine, trigeminal autonomic cephalalgias, cervicogenic headache, hemicrania continua, trigeminal neuralgia), depression, and postherpetic neuralgia.1,4–24 Stimulation technology has also been used in a case series to treat central hypoventilation syndrome by stimulation of the phrenic nerve.
This chapter focuses on complications reported during peripheral (distal) stimulation of cranial nerves, namely the terminal branches of the trigeminal nerve, the trigeminocervical complex, and the vagus nerve. Although epidural trigeminocervical complex stimulation has been reported to treat trigeminal neuralgia,25 the reader is directed to Chapter 1 for discussion of complications of epidural spinal cord stimulation (SCS).
Although a review of the American Society of Regional Anesthesia’s 2010 guidelines for neuraxial interventions may not directly be applicable to peripheral branch of cranial nerve stimulation interventions, concurrent use of anticoagulants before surgery may increase the bleeding risk. Therefore it is advised that readers familiarize themselves with these guidelines, as well as the guideline statements of perioperative use of anticoagulant therapy.26
Patient selection guides treatment success. Psychometric testing for neuromodulation candidacy deserves special mention. It is well established that concurrent psychiatric illness reduces interventional treatment success rates27 and that approximately 20% to 45% of pain patients have accompanying psychopathology.28 Therefore it is essential that appropriate measures be taken to diagnose, treat, or exclude unsuitable candidates. Instruments described to aid in identifying the presence of clinically significant psychopathology include the Symptom Checklist 90 (SCL-90-R) and the Minnesota Multiphasic Personality Inventory (MMPI-2). Poor treatment outcome was identified in patients with presurgical somatization, depression, anxiety, and poor coping.29
Background
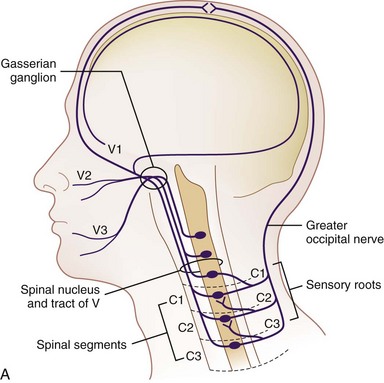
Trigeminal stimulation techniques have been described both centrally and peripherally; however, more reliable stimulation has been achieved in the latter.4 Furthermore, because overall complications of central trigeminal gasserian stimulation have been reported to be near 30% to 40%30–32 and with reduced complications with peripheral branch stimulation, enthusiasm for central stimulation has dwindled. The trigeminal nuclear systems are bilateral structures that span from the midbrain to the medulla. The caudal-most portion, the trigeminal nucleus caudalis, may extend down as far as the second or third cervical level, which has both anatomic and clinical implications. Goadsby33 demonstrated the presence of convergence between the cervical and trigeminal system, forming a trigeminocervical complex. This was characterized by Anthony34 and helped form the basis for greater occipital nerve stimulation for treatment of headache (Fig. 3-1). Traditionally, stimulation was achieved by using either implanted cylindrical or paddle leads. There are some reports of using a small implantable device without the traditional implantable pulse generator (IPG) placement10 along with transcutaneous electrical nerve stimulation unit applications.11
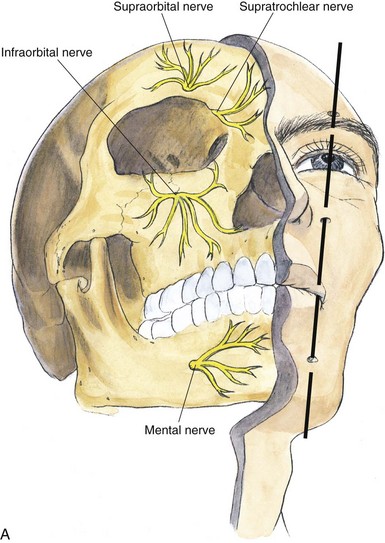
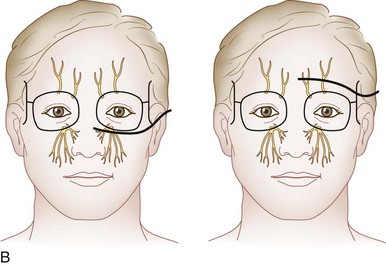
Peripherally, the trigeminal nerve terminates as the supraorbital and supratrochlear nerve from V1, the infraorbital nerve from V2, and the mental nerve from V3. These sites lend themselves to subcutaneous neurostimulatory targets (Fig. 3-2).4,6,12,17,18,24,35,36
Fig. 3-2 A, Terminal branches of the trigeminal nerve.
(From Brown DL: Atlas of regional anesthesia, ed 3, Philadelphia, WB Saunders, 2006.)
Vagal nerve stimulation (VNS) has been approved for drug-refractory epilepsy and is a viable option for those who decline surgery or nonsurgical candidates. Its safety and efficacy have been well established.37 Furthermore, it has been used in the treatment of people with treatment-resistant depression. Commonly, the left vagus nerve is stimulated, not with the commonly used spinal cord stimulator but via a NeuroCybernetic Prosthesis.38 The exact mechanism of action is unknown, although it is postulated to involve vagal sensory afferents. Whereas high-frequency stimulation causes electroencephalographic desynchronization, low-frequency stimulation causes synchronization.39 Typically, the VNS is positioned on the left side because right-sided stimulation causes more cardiac slowing as a consequence of sinoatrial (SA) node stimulation.40 Although this is not commonly used to treat pain, the scope is broadening.35,41,42 Therefore, VNS is discussed here briefly for completeness.
Selected Complications
Greater Occipital Nerve Stimulation (Table 3-1)
Lead Tip Erosion
Trentman et al43 in 2008 reported on two cases of lead erosion after greater occipital nerve stimulation occurring months after implantation. One patient was a 27-year-old woman who had intended weight loss after gastric bypass surgery of 52 kilograms; the other case did not have any identifiable risk factors, including smoking, diabetes, or infection. The authors contended that care needs to be emphasized when implanting the paddle or percutaneous electrode, not placing the lead tip too superficial or lateral, lessened by avoiding the lateral decubitus position during implant. Furthermore, extreme weight reduction or patients with very low body mass indexes may be susceptible to eventual lead migration.43
Table 3-1 Reported Greater Occipital Nerve Stimulation Complications
| Complication | Frequency |
|---|---|
| Lead tip erosion | Two reported43 |
| Lead migration | 27.3%,38 33%47* |
| Hardware malfunction | 1.7%,38 1/819 |
| Infection | 5.9%,38 2/7,65 3/166 |
| Lead fracture or disconnect | 2.6%38 |
| Allergy | 0.8%38 |
| Explant | 2.6%38 |
| Contact dermatitis | 7%47 |
| Neck stiffness | 13%47 |
| Pain over the device (IPG or lead) | 1/10,22 3/15,20 7%47 |
| Myofascial pain | 1/11,66 1/15,20 five case reports,44 7%47 |
| Battery depletion | 42% at 3 years47 |
| Stimulation tolerance | Case report53 |
| Overstimulation | 3/610 |
IPG, implantable pulse generator.
* Reported 100% lead migration at 3 years.
Management of lead tip erosion of occipital stimulation leads centers on infection management and revision. Infectious management includes assessment of extent and depth of infection. Generally, two approaches can be used: attempt to salvage the lead and system or explant and reimplant at a future date. Because many patients have greater occipital nerve stimulators secondary to a medically intractable headache, many patients request lead salvage strategies. Trentman et al43 described resection of granulomatous tissue around eroded lead and was sutured to the fascia and closed primarily along with a concurrent postoperative course of appropriately selected bacteria-sensitive antibiotics by culture.
Infection
As one can appreciate, a superficial or deep subcutaneous infection and its management, from a subcutaneously placed lead, are drastically different than an epidural abscess from an epidural lead. That being said, the potential for leads placed near the nuchal ridge can theoretically spread intracranially via the emissary veins.44 As illustrated, device salvage has been described for peripheral nerve (or peripheral branch of cranial nerve) stimulation.
Surgical site wound prevention, however, is largely the same.45 As with any surgical procedure, antimicrobial prophylaxis should occur within 30 minutes of skin incision and cover the most commonly implicated organisms. The decision to provide postoperative prophylactic antibiotics continues to be a controversial topic because many practitioners continue to do so despite only anecdotal evidence. Surgical preparation includes optimizing and mitigating patient comorbidities that increase infectious risk, ensuring proper scrub, and promoting a sterile and accessible operative field.46 Hair removal should be performed immediately before the procedure, and hair should be clipped because shaving increases the chance of infection secondary to microabrasion. Skin preparation is usually accomplished by chlorhexidine gluconate, povidone–iodine, or alcohol-based solutions. Intraoperative strategies to reduce infection include meticulous sterile technique, layered wound closure to avoid dead space, appropriate hemostasis, avoidance of placing sutures overlying the device, and nonpressured irrigation (in clean uncontaminated surgeries).
Related posts:
 Complications of Intrathecal Drug Delivery Systems
Complications of Intrathecal Drug Delivery Systems
 Radiation Safety and Complications of Fluoroscopy, Ultrasonography, and Computed Tomography
Radiation Safety and Complications of Fluoroscopy, Ultrasonography, and Computed Tomography
 Complications of Sacroiliac Joint Injection and Lateral Branch Blocks, Including Water-Cooled Rhizotomy
Complications of Sacroiliac Joint Injection and Lateral Branch Blocks, Including Water-Cooled Rhizotomy
 Complications of Lumbar Spine Fusion Surgery
Complications of Lumbar Spine Fusion Surgery
 Complications Related to Radiofrequency Procedures for the Treatment of Chronic Pain
Complications Related to Radiofrequency Procedures for the Treatment of Chronic Pain
 Complications of Therapeutic Minimally Invasive Intradiscal Procedures
Complications of Therapeutic Minimally Invasive Intradiscal Procedures

Full access? Get Clinical Tree


