Analgesia
 Respiratory depression
Respiratory depression
 Cough suppression
Cough suppression
 Nausea
Nausea
 Euphoria
Euphoria
 Dysphoria
Dysphoria
 Sedation
Sedation
 Pruritus
Pruritus
 Miosis
Miosis
 Direct bowel
Direct bowel
 RESPIRATORY DEPRESSION
RESPIRATORY DEPRESSION
Definition
Respiratory depression is most often defined as bradypnea or reduced respiratory rate. However, one of the difficulties of determining rates of respiratory depression is that there is no clear definition in the literature. It has been variously defined in different studies as hypoxia, hypoxemia, hypercarbia, hypercarbemia, or bradypnea.2,3
Scope
Respiratory depression is a well-known and widely recognized opioid effect, and the literature does not help establish a rate for the effect. The effect is dose dependent and highly sensitive to risk factors. Respiratory depression is more likely to occur during acute rather than chronic pain treatment because (i) patients are often opioid naive and (ii) other respiratory depressant drugs (hypnotics and anxiolytics) are often used concomitantly. Some degree of respiratory depression is an inevitable consequence of opioid use in opioid naive patients even at low doses. Mild respiratory depression may warrant supplementary oxygen, but is otherwise clinically unimportant. Serious respiratory depression can cause hypoxic brain injury, even death, making it the most serious adverse effect of acute opioid therapy. The effect can usually be avoided by using safe dosing protocols and appropriate monitoring.
Proposed Mechanism
The brain-stem rostral ventrolateral medulla is thought to be the main target for opioid respiratory depressant effects (Fig. 19-1). The area is the chief generator of respiratory rhythm.4–6 Exogenous opioids may reach this area from the systemic circulation, after crossing the blood-brain barrier, or from cerebrospinal fluid (CSF) in the case of neuraxial administration.
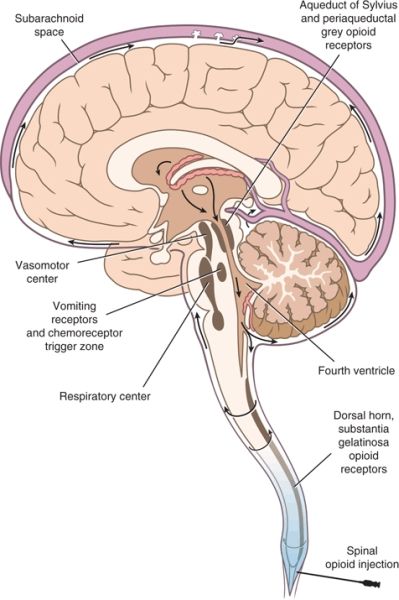
FIGURE 19-1. CSF flow diagram showing targets for spinal opioids. Drugs injected into the epidural space or intrathecal space will tend to accumulate in CSF at the level of injection. The accumulation of hydrophilic drugs such as morphine will tend to be greater than that of lipophilic drugs such as fentanyl. Slowly diffusing drugs such as morphine will be subject to bulk flow of CSF and will tend to move cephalically toward the ventricular system in the brain. Bulk CSF flow varies markedly from patient to patient. If drug does reach the ventricular system, notably the fourth ventricle, it is likely to cause respiratory depression (and possibly nausea) because the respiratory center and chemoreceptor trigger zone are at the base of the fourth ventricle. Slowly diffusing drugs will likely provide a good spread of analgesia, as the drug will spread widely to the opioid receptors concentrated in the substantia gelatinosa of the dorsal horn.
Risk Factors
Respiratory depression is more likely to occur in opioid naive patients and is therefore a particular risk in acute pain treatment. Opioid respiratory depressant effects are exacerbated by concomitant use of sedative drugs (hypnotics, anesthetics, and anxiolytics), with which they have a powerful synergistic effect. The risk of respiratory depression is also increased in the very young, the elderly, and the infirm.7 In neonates and infants, the immaturity of the nervous system (together with poor clearance) accounts for the increased sensitivity. In the elderly, increased sensitivity occurs chiefly because of poor clearance. In sick patients, a number of factors could contribute, including baseline mental status deterioration, poor clearance, and general debilitation. Other conditions associated with special risk are neuromuscular disorders, including myasthenia gravis, chronic lung disease, and sleep apnea.
Diagnostic Evaluation
Rapid-onset apnea can occur in two situations: (i) immediately after an intravenous (IV) injection of a high opioid dose, particularly of lipophilic opioids such as fentanyl or (ii) sometime after a neuraxial injection, typically of intrathecal morphine. More commonly, there is a progressive decrease in the respiratory rate before apnea occurs, and early intervention can prevent serious progression toward hypoxia or apnea. It is more important to monitor respiratory rate than oxygenation because hypoxia may not arise until late in the course of respiratory depression. Pulse oximetry serves as a useful signal for hypoxia, but is less useful as an early warning. It should be possible to preempt hypoxia by responding to decreases in respiratory rate. Practical methods for monitoring respiratory rate are direct observation and respiratory monitoring. Respiratory monitors use sensors that detect chest wall movement. Present-day multichannel monitors often incorporate respiratory monitors and use the electrocardiogram electrodes to sense the chest wall movement. Monitors that use dedicated sensors are more reliable and are sometimes used for neonates and infants in whom chest wall excursions are smaller and more sensitivity is required. Capnography can also be used to detect respiratory rate and hypercarbia, but is not usually practical for nonintubated awake patients. All monitoring equipment is subject to error, and thus the most reliable method is direct observation. During periods of high risk (e.g., early in the course of treatment), the respiratory rate should always be directly observed, even when respiratory monitors and pulse oximetry are used.
Prevention
Three approaches can be used to minimize serious complications of respiratory depression:
1. Use of safe dosing protocols, and appropriate adjustment when risk factors are present
2. Careful monitoring of respiratory depression and early intervention
3. Use of opioid-sparing analgesia regimes
Intervention
Opioid antagonists can be used to reverse opioid-induced respiratory depression, but there are drawbacks. Even small doses may reverse analgesia, so that well-controlled pain becomes agonizing. The effects of the agonist often outlive those of the antagonist, and thus there is a risk of recurrence of respiratory depression once the antagonist wears off. One recommended regime for naloxone is 0.4 mg diluted into 10 mL saline, giving 1 mL per dose while observing effects. Before giving naloxone, simple strategies such as shaking the patient, reminding them to breathe, talking to them, or otherwise stimulating them can be tried. Other analeptics such as physostigmine or flumazenil can successfully reverse respiratory depression without reversing analgesia, especially after anesthesia.
Opioid Sparing
The concept of opioid sparing began with the recognition that surgical outcome could be improved by reestablishing normal physiological function as early as possible after surgery. This meant getting patients out of bed early, removing feeding tubes and urinary catheters early, feeding early, encouraging coughing and deep breathing, and early resumption of normal activities. Many opioid effects run counter to these goals, particularly sedation and bowel effects. Opioid-sparing strategies include epidural analgesia, nerve blocks, dexmedetomidine, ketamine, and nonsteroidal anti-inflammatory drugs (NSAIDs).
There is robust evidence that, relative to IV opioids, continuous epidural analgesia has superior analgesic efficacy while reducing postoperative respiratory depression and recovery of bowel function (Table 19-1).8–16 Epidural analgesia is effective because it uses low-dose (if any) opioid in the epidural space, which in turn has limited systemic absorption. Spinal analgesia is thus maximized, whereas undesirable systemic effects such as respiratory depression, sedation, nausea, and bowel slowing are minimized. Extended-release epidural morphine may be an exception to this principle, with one recent meta-analysis showing more respiratory depression compared with parenteral opioids.17
TABLE 19.1 Key Studies Validating the Ability of Epidural Analgesia to Reduce Respiratory Depression
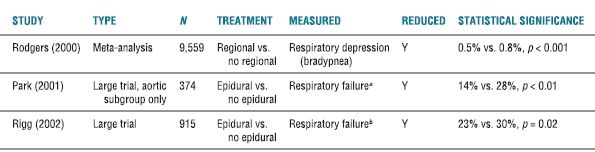
Note: All control group patients received systemic opioid for postoperative analgesia.
aRespiratory failure is defined here as the need for intubation and mechanical ventilation for more than 24 h postoperatively or the need for reintubation and mechanical ventilation after 1 h postoperatively.
bRespiratory failure is defined here as the need for ventilation beyond 1 h after surgery or reintubation; PaO2 ≤ 50 mm Hg; or PaCO2 ε 50 mm Hg.
Ketamine is an NMDA (N-methyl-d-aspartic acid) receptor antagonist that functions clinically as a dissociative anesthetic with analgesic properties. Its principal negative side effects are dose-dependent psychomimetic symptoms, specifically vivid dreams, hallucinations, and delirium. Subanesthetic doses of ketamine given perioperatively consistently reduce the total dose of opioid for postoperative pain.18–25 In contrast, single dose of pre-incision ketamine has little clinical benefit with respect to opioid sparing in the first two postoperative days and opioid-related side effects.26,27 A 2005 Cochrane review found that 27 of 37 included trials showed that perioperative ketamine reduced 24-hour opioid dose as well as nausea and vomiting, with minimal or absent side effects.28 Unfortunately, respiratory depression per se was not studied. “Sedation scores,” however, were significantly increased in the ketamine group in the first 2 to 4 hours postoperatively, with no difference in the ketamine- and non–ketamine-treated groups thereafter. Thoracic surgery patients may have particular benefit with ketamine reducing opioid-related respiratory depression. Compared to morphine patient-controlled analgesia (PCA) alone, the combination of morphine and ketamine PCA reduced both the postoperative pain scores and oxygen desaturation frequency.18–20 No adverse psychomimetic effects were reported from the ketamine in these studies. Patients undergoing abdominal22,23,29 and orthopedic surgery21,24 also have shown lower incidence of nausea and improved pain scores compared to morphine PCA alone with minimal ketamine-related side effects. A separate audit of 1,026 patients from a wide variety of surgical populations who received morphine and ketamine in a 1:1 weight ratio for postoperative pain found that the incidence of vivid dreams and/or hallucinations was 6.2% and respiratory depression (bradypnea, RR < 8/min for 10 minutes) was 1.2%.30 Subanesthetic doses of ketamine, therefore, constitute a safe and effective means of reducing the total opioid dose and opioid-induced respiratory depression in certain patient populations.
Dexmedetomidine and clonidine are centrally acting alpha-2 adrenergic receptor agonists used in anesthetic practice for their sedative and analgesic properties. These drugs tend to produce bradycardia and hypotension, which can be therapeutic. At high dose, or in sensitive individuals (e.g., neonates and children), respiratory depression can occur secondary to central nervous system (CNS) depression.31–34 With appropriate dosing, the agents typically produce sedation, amnesia, and mild analgesia with minimal respiratory depression.35 Dexmedetomidine is given intravenously, whereas clonidine is often given neuraxially, but may also be given orally, transdermally, or intraarticularly. In terms of opioid sparing, IV dexmedetomidine has two major roles, first as an adjunct sedative/analgesic during procedural sedation and second as an adjunct analgesic for the treatment of perioperative pain. Opioid sparing during the immediate postoperative period after pre-induction or intraoperative dexmedetomidine has been demonstrated in multiple trials, although the effect does not persist into the first postoperative day.36–43 There may also be a role for postoperative dexmedetomidine. For example, a randomized controlled trial of 100 women undergoing total abdominal hysterectomy, dexmedetomidine (5 μg/mL)/morphine (1 mg/mL) PCA was superior to morphine PCA alone for postoperative analgesia with respect to pain scores, opioid use, nausea, and vomiting, with no difference in respiratory depression or sedation and lower heart rate and mean blood pressure.44 Like dexmedetomidine, clonidine has been shown to enhance analgesia and reduce opioid doses in the perioperative period when given neuraxially,31,45–48 orally,49 and intraarticularly.50,51 Data on clonidine reducing opioid-related side effects are more limited. Overall, the alpha-2 receptor agonists do appear to have useful analgesic and opioid-sparing effects, although as with many sedating drugs used as adjuncts to opioids, their ability to reduce opioid-induced respiratory depression per se may be less certain.
NSAIDs have also been studied as opioid-sparing analgesic adjuncts. Without question, NSAIDs reduce to the total dose of narcotic required for pain relief.52–58 With respect to reducing respiratory depression, however, the literature is more equivocal with only selected trials showing decreased rates of respiratory depression.52,54,56,58
Peripheral nerve blocks, like epidural analgesia, offer excellent treatment of acute pain with minimal to no opioid supplementation. Numerous studies have demonstrated that peripheral nerve blockade is an effective means of opioid sparing following extremity surgery59–61 and certain types of abdominal surgery, specifically open appendectomy, cesarean section, and hysterectomy.62–64 Unfortunately, peripheral nerve blocks are not an option for many types of abdominal and thoracic surgery. Even for surgery on the upper and lower extremities, catheters frequently become dislodged requiring replacement or opioid supplementation, thus limiting their benefit with frequent reliance on opioids for acute postoperative pain. Nonetheless, a recent meta-analysis of femoral nerve blocks for knee arthroscopy with 10 studies and 1,016 patients showed that even a single-shot femoral nerve block significantly reduced nausea, postoperative pain scores at 24 and 48 hours and 12- and 24-hour postoperative morphine consumption.61 There was no difference in sedation scores between parenteral opioids alone, single-shot femoral nerve block, and continuous femoral nerve blockade. Thus, where feasible, peripheral nerve blockade may be a useful option to reduce opioid consumption for postoperative analgesia. Their ability to reduce opioid-related respiratory complications, however, remains unproven.
Summary
Respiratory depression is a potentially dangerous opioid effect that is especially likely to occur during systemic opioid treatment of acute pain. The use of safe dosing protocols, knowledge of risk factors, use of appropriate monitoring, early intervention, and use of opioid-sparing techniques can help minimize related complications.
 OVERDOSE
OVERDOSE
Scope
The chief reason for avoiding overdose is to avoid respiratory depression. Dosing errors arise for a number of reasons (Box 19-2). Most dosing errors are human errors; some are system errors. The introduction of standardized protocols and especially the use of computerized systems with coding for ordering, distributing, and delivering medications has markedly reduced both human and system medication errors.65,66
BOX 19-2 Causes of Opioid Dosing Errors
 Failure to follow recommended dosing protocol
Failure to follow recommended dosing protocol
 Lack of knowledge of risk factors, failure to recognize existence of risk, and/or failure to adjust dose according to risk
Lack of knowledge of risk factors, failure to recognize existence of risk, and/or failure to adjust dose according to risk
 Calculation errors
Calculation errors
 Misreading orders
Misreading orders
 Lack of familiarity with treatment
Lack of familiarity with treatment
 Pharmacy errors
Pharmacy errors
Prevention
A question that must arise is whether the use of PCA can reduce the incidence of respiratory depression by reducing the likelihood of inappropriate dosing. PCA does have intrinsic safety in that small and frequent doses are used and the patient controls dosing (Fig. 19-2). Provided dosing parameters are set correctly and the method is used correctly (i.e., without being overridden by anyone other than the patient), patients are unlikely to receive an overdose because they will usually stop activating the pump when they are obtunded. Conventional methods are thought to be less safe because larger doses are given less often. Slow absorption from intramuscular (IM) or subcutaneous (SC) deposit sites makes IM and SC administration safer than IV administration during conventional dosing, but it is still possible to absorb suprathreshold doses after the onset of obtundation.
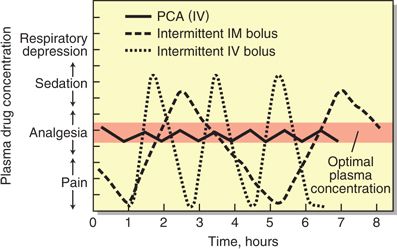
FIGURE 19-2. Relationship between the plasma drug concentration and pharmacologic effect of opioid analgesics over time when administered using various methods: PCA (patient-controlled analgesia), IV (intravenous), and IM (intramuscular).
Despite the theoretical advantage of PCA in terms of safety and avoidance of overdose, there is little support in the literature for superior safety. Two meta-analyses, one published in 199367 and the other in 2001,68 failed to show any superiority for PCA in terms of adverse effects. Fifteen trials (787 patients) were included in the first analysis and 32 trials (2,072 patients) in the second. The first meta-analysis was able to show convincingly that patients prefer PCA to conventional analgesia and that PCA has slightly better analgesic efficacy. The mean difference in satisfaction was 42% (p = 0.02), whereas the mean difference in pain score on a scale of 0 to 100 was 5.6 (p = 0.006). However, there was no difference in opioid usage, adverse effects (including respiratory depression), or length of hospital stay. Most recently, in 2006, a systematic Cochrane review of patient-controlled IV opioids versus conventional, as needed IV opioid analgesia, confirmed the findings of the previous two meta-analyses.69 Despite the passing of almost 20 years, and the addition of 38 trials (3,074 patients) to the first meta-analysis, the results of the third analysis differ very little from either the first or the second. Thus, patients’ preference for PCA was confirmed, as was slightly better analgesic efficacy. There was no difference in adverse effects (including respiratory depression), and no convincing evidence of a difference in surgical outcome. A Canadian review of 1,600 charts of patients receiving PCA after surgery found eight cases of respiratory depression.70 Factors associated with respiratory depression (Box 19-3) were the use of a background infusion (in addition to patient-controlled boluses), concomitant use of sedatives, and a history of sleep apnea. None of the cases were due to operator error or equipment malfunction.
BOX 19-3 Factors Associated with Respiratory depression during use of PCA
 Use of background (basal) infusions in addition to patient-controlled boluses
Use of background (basal) infusions in addition to patient-controlled boluses
 Concomitant use of sedatives
Concomitant use of sedatives
 History of sleep apnea
History of sleep apnea
Related posts:

Full access? Get Clinical Tree


