DEFINITION AND SCOPE
The relevant anatomy and technique for superior hypogastric and ganglion impar blocks have been well described, but only limited observational data point to the usefulness of these techniques for treating pain arising from the pelvic viscera. Few complications have been reported as resulting from these techniques. Therefore, much of the following discussion focuses on potential complications.
Stretch, compression, invasion by tumor, or distension of visceral structures can result in a poorly localized noxious type of pain known as visceral pain. Patients experiencing visceral pain often describe the pain as vague, deep, squeezing, crampy, or colicky. Other signs and symptoms include referred pain (e.g., shoulder pain that appears when the liver’s capsule of Gleason is distended due to tumor growth) and nausea/vomiting due to vagal irritation.
Visceral pain associated with cancer may be relieved with oral pharmacologic therapy that includes combinations of nonsteroidal anti-inflammatory drugs, opioids, and other adjuvant therapy. In addition to pharmacologic therapy, neurolytic blocks of the superior hypogastric plexus are also effective in controlling pelvic visceral pain due to cancer and should be considered as important adjuncts to pharmacologic therapy for the relief of severe pain experienced by cancer patients. These blocks rarely eliminate cancer pain, because patients frequently experience coexisting somatic and neuropathic pain. Therefore, oral pharmacologic therapy must be continued in the majority of these cases, albeit at lower doses. The goals of performing a neurolytic block of this nature are to maximize the analgesic effects of opioid or nonopioid analgesics while reducing the total daily dose of these agents to alleviate or reduce both the incidence and the severity of side effects.
 SUPERIOR HYPOGASTRIC PLEXUS BLOCK
SUPERIOR HYPOGASTRIC PLEXUS BLOCK
Cancer patients with tumors within the organs of the pelvis may experience severe pain that is unresponsive to oral or parenteral opioids. Moreover, excessive sedation or other side effects may limit the acceptability and usefulness of oral opioid therapy and/or adjuvants. Therefore, an invasive approach that effectively controls pain would improve the quality of life of these patients.
Clinical Uses
Visceral pelvic pain associated with cancer and chronic nonmalignant conditions may be alleviated by blocking the superior hypogastric plexus.1,2 Analgesia is possible because the afferent fibers innervating the organs in the pelvis travel in the sympathetic nerves, trunks, ganglia, and rami. Thus, a sympathectomy for visceral pain is analogous to a peripheral neurectomy or dorsal rhizotomy for somatic pain. A recent study1 suggests that visceral pain is an important component of the cancer pain syndrome experienced by patients with cancer of the pelvis, even in advanced stages. Thus, percutaneous neurolytic blocks of the superior hypogastric plexus should be considered more often for patients with advanced stages of pelvic cancer.
Anatomy
The superior hypogastric plexus is situated in the retroperitoneum, bilaterally extending from the lower third of the fifth lumbar vertebral body to the upper third of the first sacral vertebral body (Fig. 24-1). It receives fibers from the inferior hypogastric plexus, which in turn receives all afferent fibers from the pelvic organs. Because the inferior hypogastric plexus is not a distinct structure, but rather a group of branched fibers, it would be difficult to perform a neurolytic procedure at this level. Conversely, the superior hypogastric plexus has two well-defined ganglia, making it feasible to block.
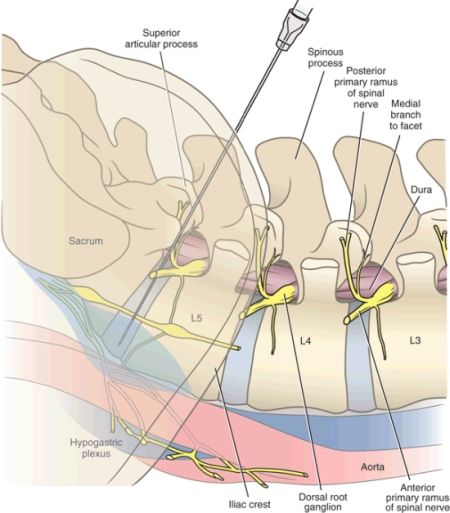
FIGURE 24-1. Anatomy of the superior hypogastric plexus. The superior hypogastric plexus is comprised of a loose web-like group of interlacing nerve fibers that lie over the anterolateral surface of the L5 vertebral body and extend inferiorly over the sacrum. Needles are positioned over the anterolateral surface of the L5/S1 intervertebral disc of the inferior aspect of the L5 vertebral bodies to block the superior hypogastric plexus. (Reproduced with permission from Rathmell JP. Atlas of Image-guided Intervention in Regional Anesthesia and Pain Medicine. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins,2012.)
Technique
Patients are placed in the prone position with a pillow under the pelvis to flatten the lumbar lordosis. Two 7-cm needles are inserted with the bevel directed medially 45 degrees and 30 degrees caudad so that the tips lie anterolateral to the L5-S1 intervertebral disc space. Aspiration is important to avoid injection into the iliac vessels. If blood is aspirated, a transvascular approach can be used. The accurate placement of the needle is verified via biplanar fluoroscopy. Anterior-posterior (AP) views should reveal the tip of the needle at the level of the junction of the L5 and S1 vertebral bodies. This is an important safety step to avoid potential spread of the neurolytic agent toward the L5. Lateral views will confirm the placement of the needle’s tip just beyond the vertebral body’s anterolateral margin. The injection of 3 to 5 mL of water-soluble contrast medium is used to verify the accurate needle placement and to rule out intravascular injection. In the AP view, the spread of contrast should be confined to the midline region. In the lateral view, a smooth posterior contour corresponding to the anterior psoas fascia indicates that the needle is at the appropriate depth. Figures 24-2 and 24-3 show adequate needle placement and contrast medium spread prior to neurolysis of the superior hypogastric plexus.
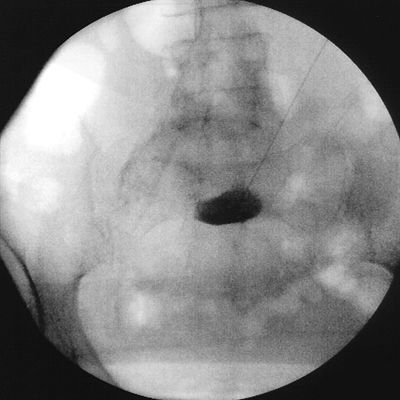
FIGURE 24-2. Superior hypogastric plexus block. Anteroposterior view of the lumbosacral area with a 22-gauge Chiba needle placed at the junction of the lumbosacral vertebrae. Notice that the injection of 3 mL of radiographic contrast was performed with a single needle to demonstrate the spread to the midline.

FIGURE 24-3. Superior hypogastric plexus block. Cross-lateral view of the lumbosacral region with two 22-gauge Chiba needles placed at the correct site and one placed in the upper third of the fifth lumbar vertebra. This last needle represents inappropriate needle placement.
For a prognostic hypogastric plexus blockade or for patients with non–cancer-related pain, local anesthetic alone is used. For therapeutic purposes in patients with cancer-related pain, phenol is typically used as the neurolytic solution.
The transdiscal approach has gained interest as an alternative to the classic approach for some patients. Barriers to the classic approach to the superior hypogastric plexus block (SHPB) include atherosclerotic disease of the iliac vessels, the L5 transverse process, the L5 nerve root, and the iliac crest. Two transdiscal approaches have been described—a traditional lateral approach that is performed similar to discography at the L5-S1 level3 and a posteromedian approach that involves crossing the subarachnoid space.4 Figures 24-4 and 24-5 illustrate needle placement for the transdiscal approach of the SHPB in the oblique and lateral views, respectively. Figure 24-5 demonstrates the spread of contrast in the retroperitoneal space where the superior hypogastric plexus lies.

FIGURE 24-4. Superior hypogastric plexus block, transdiscal approach. Oblique view of the lumbosacral spine with localizing marks indicating the insertion site and path for a transdiscal approach to the superior hypogastric plexus.

FIGURE 24-5. Superior hypogastric plexus block, transdiscal approach. Lateral view of the lumbosacral area with a 22-gauge needle penetrating the L5/S1 disc. Note that the injection of 3 mL of contrast demonstrated spread in the retroperitoneum from the caudal half of the L5 vertebral body to the cephalad one-third of the S1 vertebral body.
Gamal et al.3 compared the classic and transdiscal approach to the SHPB in 30 patients and reported that the transdiscal approach was associated with decreased procedure time, similar efficacy, and no complications. Despite lack of complications reported, the limited data available combined with recent data concerning long-term complications of discography raise some concerns for routine use of this approach.
The anterior approach to the SHPB has also been described using either CT guidance or ultrasound.5,6 Prior to attempting an anterior approach to the SHPB, patients need to have preprocedure bowel and bladder preparation to limit the risk of visceral injury and possible intraabdominal or retroperitoneal infection. A case series of 10 patients reported that a CT-guided anterior approach is a safe and effective alternative approach for performing an SHPB.5 This technique allows for detailed visualization of the aorta, iliac veins, and lumbar nerve roots, but it does involve inserting a needle through intestinal loops, which can result in transmitting intestinal flora to the retroperitoneum.
Efficacy
The effectiveness of the block was originally demonstrated by documenting a significant decrease in pain via visual analog pain score (VAPS). In this study, Plancarte et al.2 showed that the block was effective in reducing VAPSs in 70% of patients with pelvic pain associated with cancer. The majority of the enrolled patients had cervical cancer. In a subsequent study, 69% of patients experienced a decrease in VAPSs. Moreover, a mean daily opioid (morphine) reduction of 67% was seen in the success group (736 ± 633 reduced to 251 ± 191 mg/d) and 45% in the failure group (1,443 ± 703 reduced to 800 ± 345 mg/d).1 In a more recent multicenter study, 159 patients with pelvic pain associated with cancer were evaluated. Overall, 115 patients (72%) had satisfactory pain relief after one or two neurolytic procedures. Mean opioid use decreased by 40% from 58 ± 43 reduced to 35 ± 18 equianalgesic mg/d of morphine 3 weeks after treatment in all the studied patients. This decrease in opioid consumption was significant for both the success group (56 ± 32 reduced to 32 ± 16 mg/d) and the failure group (65 ± 28 reduced to 48 ± 21 mg/d).7 Success was defined in these two studies as the ability to reduce opioid consumption by at least 50% in the 3 weeks following the block and a decrease to <4/10 in the VAPSs.1,7
In a recent case report, Rosenberg et al.8 reported on the efficacy of this block in a patient with severe chronic nonmalignant penile pain after transurethral resection of the prostate. Although the patient did not receive a neurolytic agent, a diagnostic block performed with 0.25% bupivacaine and 20 mg of methylprednisolone acetate was effective in relieving the pain for >6 months. The usefulness of this block in chronic benign pain conditions has not been adequately documented in a large cohort of patients.
Complications: Mechanism, Risk Factors, Treatment, and Prevention
The combined experience of more than 200 cases from the Mexican Institute of Cancer, Roswell Park Cancer Institute, and M.D. Anderson Cancer Center indicates that neurologic complications do not occur as a result of this block.7 However, inadequate needle placement may lead to catastrophic results, as suggested by the fluoroscopy images shown in Figures 24-6 and 24-7. In this case, one of the needles was placed in the superior third of L5 and after injection of contrast medium, posterior extension with delineation of the L5 nerve root was noted. The tip of needle needs to be placed in the inferior third of L5 to avoid this potential problem. Moreover, careful evaluation of the postcontrast medium injection images must be done to rule out abnormal spread.
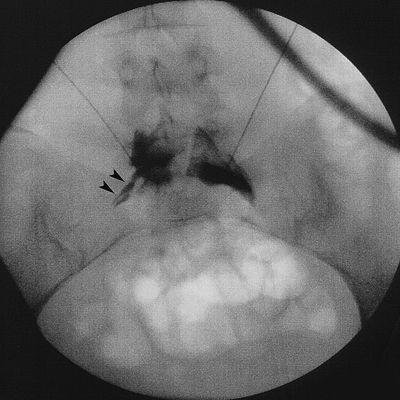
FIGURE 24-6. Superior hypogastric plexus block. Anteroposterior view of the lumbosacral area with a 22-gauge Chiba needle placed at the upper third of the fifth lumbar vertebra. Note that the injection of 3 mL of radiographic contrast resulted in posterior spread to the L5 spinal nerve (arrowheads). Injection of neurolytic solution in the position is likely to lead to direct neural injury to the L5 spinal nerve, with partial sensory and motor loss in the lower extremity.



