Chapter 12 Complications Associated with Head and Neck Blocks, Upper Extremity Blocks, Lower Extremity Blocks, and Differential Diagnostic Blocks






Introduction
As with any medical procedure, the physician performing the procedure should weigh the benefits versus the risks. Interventional procedures have significant potential benefit for those suffering from chronic pain. Although uncommon, complications may result in catastrophic outcomes. This chapter reviews the complications associated with a diverse group of procedures, including head and neck blocks, upper extremity blocks, lower extremity blocks, and differential diagnostic blocks. The complications associated with these can generally be divided into vascular, infectious, neural, pharmacologic, and anatomically related to the specific sight of injection (Table 12-1).
Table 12-1 Overview of Complications Associated with Head and Neck Block, Upper Extremity Block, Lower Extremity Block, and Differential Diagnostic Block Procedures
| Vascular1–6 | |
| Infectious | |
| Pharmacologic | |
| Neural2,14–16 |
CNS, central nervous system.
Vascular
Many neural structures are intimately connected with vasculature. Overall, the likelihood of a vascular complication is rare but potentially devastating. Reported vascular complications include airway, neural, and microvascular compression related to hematoma formation.1–3 Additionally, arterial dissection, pseudoaneurysm, and vascular insufficiency secondary to vasospasm have all been cited in the literature.4–6
Infection
The likelihood of infection from any single injection is extremely rare. Infection requiring intervention after an indwelling catheter has been reported as high as 0.8%.7 With interventional procedures involving the neuraxis, terrible sequelae, including epidural abscess or meningitis, may occur. Evidence demonstrates that catheter insertion (particularly >48 hours), intensive care unit admission, male sex, lack of prophylactic antibiotics, and lack of provider experience increase the likelihood of infection.8
Local Anesthetic Toxicity
The proximity of many neural structures to major vessels predisposes itself to the potential for local anesthetic toxicity. Inadvertent vascular puncture is the most likely cause of toxicity, but it has been suggested that with no identifiable puncture, clinical doses may cause toxicity.9 It appears that clinically significant local anesthetic toxicity occurs between 7.5 and 20 times per 10000 regional anesthetics.10 Local anesthetic toxicity can be categorized by symptoms involving the central nervous system (CNS) and those related to cardiovascular toxicity (Table 12-2).
Table 12-2 Signs and Symptoms Associated with Local Anesthetic Toxicity
| Central nervous system11 | |
| Cardiovascular12 |
CNS, central nervous system.
Neurologic
The likelihood of long-term neurologic injury is low, reported below 0.02%.13 When these injuries do occur, the outcome is often devastating to the clinician and patient alike. Nerve injury may present in a spectrum from paresthesias to paralysis, with neuropathic pain being a dreaded outcome.
Etiologies attributed to nerve injury include direct needle trauma, barotrauma from high-pressure injection, compression from hematoma, and local anesthetic neural toxicity.2,14–16
Complications of Head and Neck Blocks
A variety of percutaneous techniques are available for targets at head and neck, including sphenopalatine ganglion (SPG), Gasserian ganglion, atlantoaxial joint (AAJ) and atlantooccipital joint (AOJ), stellate ganglion, and C2 dorsal root ganglion. See Table 12-3 for a description of complications associated with head and neck injections.
Table 12-3 Common Head and Neck Blocks with Associated Complications
| Gasserian ganglion block and neurolysis17,32 | |
| SPG block20–24 | |
| AAJ and AOJ injections19 | |
| Stellate ganglion block1,33,34 | |
| C2 dorsal root ganglion injection |
AAJ, atlantoaxial joint; AOJ, atlantooccipital joint; CSF, cerebrospinal fluid; PPF, pterygopalatine fossa; RFA, radiofrequency ablation; SPG, sphenopalatine ganglion.
Gasserian Ganglion Block and Neurolysis
The Gasserian (trigeminal) ganglion lies within the Meckel cave, which contains cerebrospinal fluid (CSF), and local anesthetic deposited in this area may spread to other cranial nerves and can potentially cause brainstem anesthesia.17 Infection, CSF leak, bleeding, and nerve damage are also likely with Gasserian ganglion block or ablation because it is located in the middle of the brain surrounded by blood vessels. Literature studies show that RFA of the Gasserian ganglion is associated with the highest incidence of complications, with nearly one-third of patients developing some form of complications.18 Postoperative trigeminal sensory loss affects virtually all patients treated with RFA, and it is considered a side effect rather than a complication.
Sphenopalatine Ganglion Block
Epistaxis is more frequent with an intranasal approach to SPG block; intravascular injection or hematoma formation can occur after maxillary artery injury, which lies within the pterygopalatine fossa (PPF). Cheek hematoma is the most common complication. Infection is always possible especially with inadvertent needle entry into the nasal or oral cavity.19 Reflex bradycardia is likely with RFA because of the rich parasympathetic connections to the SPG.20 RFA of the SPG can result in permanent or temporary hyperesthesia or dysesthesia in the palate, maxilla, or posterior pharynx.21–23 Temporary diplopia, which is more common after local anesthetic injections rather than RFA, is caused by the spread of the injectate from the PPF to the inferior orbital fissure containing the abducent nerve.24 Temporary diplopia is likely if the needle tip is deep inside the PPF and the volume of injectate is greater than 1 to 2 mL.
Atlantoaxial Joint and Atlantooccipital Joint Injections
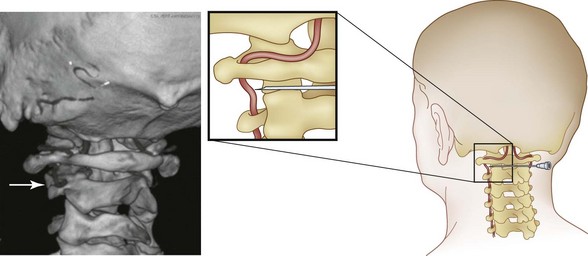
The AAJ and AOJ are in very close proximity to the vertebral artery (Fig. 12-1). Consequently, particular attention should be paid to avoid intravascular injection because vertebral artery anatomy can be unpredictable. Intraarterial injection may cause seizure or posterior circulation stroke.25 Inadvertent puncture of the C2 dural sleeve with CSF leak or high spinal spread of the local anesthetic may occur with AAJ injection if the needle is directed too medially. This can result in a rapid and profound decrease in blood pressure followed by apnea and death. Therefore, intravenous access should be established before the procedure. Spinal cord injury and syringomyelia are potential serious complications if the needle is directed even further medially.19
Stellate Ganglion Block
Many important structures lie close to the stellate ganglion. Hence, technical complications from injury to the nerves and viscera are possible during insertion of the needle.17,26,27 This includes injury to the brachial plexus; trauma to the trachea and esophagus; injury to the pleura and lung (pneumothorax, hemothorax, which may require chest tube insertion); and bleeding and local hematoma, especially if the patient was taking anticoagulants. This can lead to airway compression (Fig. 12-2).28,29 Vasovagal attacks can also occur, especially with inadvertent manipulation of carotid sinus during the block. Infectious complications are possible if there was a breach in the aseptic barrier. These can include local abscess, cellulitis, and osteitis of the vertebral body and transverse process.30

Related posts:
 Complications of Intrathecal Drug Delivery Systems
Complications of Intrathecal Drug Delivery Systems
 Radiation Safety and Complications of Fluoroscopy, Ultrasonography, and Computed Tomography
Radiation Safety and Complications of Fluoroscopy, Ultrasonography, and Computed Tomography
 Complications of Sacroiliac Joint Injection and Lateral Branch Blocks, Including Water-Cooled Rhizotomy
Complications of Sacroiliac Joint Injection and Lateral Branch Blocks, Including Water-Cooled Rhizotomy
 Complications of Lumbar Spine Fusion Surgery
Complications of Lumbar Spine Fusion Surgery
 Complications Related to Radiofrequency Procedures for the Treatment of Chronic Pain
Complications Related to Radiofrequency Procedures for the Treatment of Chronic Pain
 Complications of Therapeutic Minimally Invasive Intradiscal Procedures
Complications of Therapeutic Minimally Invasive Intradiscal Procedures

Full access? Get Clinical Tree


