COMMON OPIOID-RELATED ADVERSE EFFECTS
Common opioid-related adverse effects include constipation, urinary retention, sedation, delirium, dry mouth, respiratory depression, hyperhidrosis, pruritus, muscular spasm, tremor, nausea, and vomiting. The use of opioid analgesics is associated with these side effects, which are so common they are considered an expected part of therapy. In some cases, tolerance develops and side effects diminish. In others, side effects persist for the duration of therapy. Some or all of these side effects are present in almost all patients receiving chronic opioid therapy. The exact group of side effects and their relative severity is highly variable, individual, and drug and dose dependent.
In a systematic review of 34 randomized trials, Moore and McQuay1 examined the prevalence of adverse events related to oral opioid administration. The trials were of relatively short duration, with only two trials longer than 4 weeks and only one as long as 8 weeks. Although the trials are of relatively short duration, they are characteristic of the vast majority of literature used to support the use of opioids in treating chronic pain. The authors found that 51% of all patients taking oral opioids experienced at least one adverse event and that 22% of patients discontinued therapy due to adverse events, including dry mouth, nausea, constipation, dizziness, drowsiness or somnolence, pruritus, or vomiting (Box 34-1). The pathophysiology of these side effects is related to direct effects on opioid receptors in the brain, spinal cord, peripheral nervous system, and gut.
BOX 34-1 Common Opioid-related Adverse Effects and Their Estimated Incidence During Oral Administration
 22% of patients discontinued therapy due to adverse events
22% of patients discontinued therapy due to adverse events
 25% dry mouth
25% dry mouth
 21% nausea
21% nausea
 15% constipation
15% constipation
 14% dizziness
14% dizziness
 14% drowsiness or somnolence
14% drowsiness or somnolence
 13% pruritus
13% pruritus
 10% vomiting
10% vomiting
From Moore RA, McQuay HJ. Prevalence of opioid adverse events in chronic non-malignant pain: systematic review of randomized trials of oral opioids. Arthritis Res Ther 2005;7:R1046–R1051.
Constipation
Scope
Constipation related to the use of opioid analgesics is the most common adverse effect of chronic opioid therapy and usually requires some form of treatment, either dietary or medical.2 In the rare circumstance in which chronic diarrhea is present, reduction in bowel motility may be a welcome relief. However, in most cases, this is an undesirable side effect that should be anticipated and requires active treatment.
Pathophysiology
Opioids impair normal bowel function by binding to intestinal µ-opioid receptors and interrupting the normal coordinated rhythmic contractions required for intestinal motility. Opioids can also alter intestinal fluid secretion by a direct effect on the enteric nervous system. These actions are often accompanied by decreased gastric emptying, abdominal cramping, spasm, and bloating, and usually result in decreased frequency of bowel movements, formation of hard, dry stools, painful defecation, and incomplete bowel evacuation. In addition, peripheral actions of opioids on the gut may contribute to nausea and vomiting.
Diagnosis
Constipation is typically diagnosed on the basis of history alone. In some cases, constipation may be severe and evidence gathered through the use of abdominal x-ray, but this is the exception rather than the rule. Finally, the use of the hydrogen breath test to assess gastrointestinal transit time has been used in the research setting and in advanced gastrointestinal evaluations, but does not have wide use as a means of diagnosing constipation in the clinical setting.3
Prevention/Treatment
In the case of opioid-induced constipation, prevention and treatment are almost simultaneous. When chronic opioid therapy is initiated, it should be assumed that constipation is likely to occur and treatment should be initiated. Initial treatment may be limited to dietary changes such as increased liquid, dietary fiber, and fruit intake. If dietary changes are insufficient, use of a stool softener such as docusate sodium, promotility compounds such as senna, osmotic agents such as polyethylene glycol, and bulk agents such as methylcellulose may be used alone or in combination to reduce constipation.2,4,5
Future treatments using opioid antagonists such as alvimopan and methylnaltrexone that act to block opioid receptors in the gut without affecting opioid analgesia may offer improved treatment of this side effect. In a study by Paulson et al.6 examining the use of alvimopan in a 21-day trial of treatment for opioid-induced bowel dysfunction, the authors demonstrated significant efficacy in the management of opioid-induced bowel dysfunction. Over the 21-day treatment period, 54%, 43%, and 29% had a bowel movement within 8 hours of administration of 1.0 or 0.5 mg of alvimopan versus placebo. A more recent study by Jansen et al. examined the use of alvimopan in a randomized, placebo-controlled trial for opioid-induced bowel dysfunction in patients with noncancer pain. The primary efficacy endpoint was the proportion of patients experiencing at least three spontaneous bowel movements (SBMs; bowel movements with no laxative use in the previous 24 hours) per week over the treatment period and an average increase from baseline of at least one SBM per week. A significantly greater proportion of patients in the alvimopan 0.5 mg twice-daily group met the primary endpoint compared with placebo (72% vs. 48%, p < 0.001). Treatment with alvimopan twice daily also improved other symptoms such as stool consistency, straining, incomplete evacuation, abdominal bloating, abdominal pain, and decreased appetite compared with placebo. The opioid-induced bowel dysfunction Symptoms Improvement Scale (SIS) responder rate was 40.4% in the alvimopan 0.5 mg twice daily group, versus 18.6% with placebo (p < 0.001). Active treatment with alvimopan did not increase the requirement for opioid medication or increase average pain intensity scores.7
Sedation/Delirium
Scope
Sedation is commonly observed during initiation of opioid therapy or when significant dose increases are made.8 It is often associated with transient drowsiness or cognitive impairment. These symptoms usually resolve after a few days, and reassurance and recommendation to avoid alcohol or driving at the initiation of therapy are sufficient. In most cases, patients receiving stable doses of medication do not have significant impairment in cognitive or driving ability compared to patients not taking opioids.9,10 However, in some cases, symptoms persist and may be related to other comorbidities or the concomitant use of other sedating medications. Delirium is an acute confusional state that leads to a disturbance of consciousness and comprehension. Although sedation, mild cognitive impairment (or even hallucinations) frequently occur when opioids are started or when significant dose increases are implemented, the differential diagnosis of opioid-induced delirium is often complicated.
Pathophysiology
The pathophysiology of sedation or delirium occurring with opioid administration is related to the effects of opioids and their metabolites on receptors in the brain and spinal cord. Factors such as renal dysfunction, hepatic dysfunction, chronic high-dose opioids, preexisting cognitive impairment, dehydration, concurrent administration of other psychoactive drugs, smoking cessation, or terminal illness may all contribute to the development of delirium.
Risk Factors
Risk factors for sedation associated with the use of opioid analgesics include opioid naiveté, rapid dose increases, renal insufficiency, hepatic insufficiency, administration with other sedative medications, and concurrent metabolic disorders (Box 34-2). The relative risk of one opioid producing delirium over another is not well documented, although meperidine (with its toxic metabolite normeperidine) has been singled out as a particularly dangerous compound. The route of administration and the lipophilicity of the opioid have been suggested as potential risk factors.
BOX 34-2 Risk Factors for Sedation in Association with the Use of Opioid Analgesics
 Opioid naiveté
Opioid naiveté
 Rapid dose escalation
Rapid dose escalation
 Renal insufficiency
Renal insufficiency
 Hepatic insufficiency
Hepatic insufficiency
 Administration with other sedative medications
Administration with other sedative medications
 Concurrent metabolic disorders
Concurrent metabolic disorders
Diagnosis
Diagnosis of the causes of sedation, cognitive dysfunction, or delirium should include a careful history to elicit the temporal relationship between opioid administration and altered mental function. In addition, assessment should include evaluation of potential coexisting conditions such as dementia, renal insufficiency, metabolic encephalopathies, brain metastases, and concurrent administration of other pharmacologic agents with central nervous system activity. For instance, undesirable effects following acute overdose, after a significant dose increase and after changing to a new drug, may be related to the drug itself. In contrast, gradual onset of sedation or delirium in the setting of worsening renal insufficiency may be the result of toxic metabolite accumulation.
Prevention
Prevention of sedation/delirium may be accomplished by limiting the initial dose and rate of dose escalation and avoiding administration of these compounds to patients with limited ability to metabolize them or excrete the metabolites. In addition, choosing agents with less risk of toxic metabolite accumulation may be beneficial. Opioids may be excreted in the parent form by the kidneys. However, those that are not readily eliminated in this fashion are metabolized to form more water-soluble metabolites. Those patients with impaired renal function, including most elderly individuals and those receiving high-dose or long-term opioid therapy, are at particular risk. Normeperidine, a metabolite of meperidine, causes neurotoxicity—especially in elderly patients and those with poor renal function. Its use for acute pain should be limited to 1 to 2 days, and it should be avoided in the management of chronic pain.
Morphine-3-glucuronide and morphine-6-glucuronide are the two major water-soluble morphine metabolites dependent on renal elimination.11 Morphine-3-glucuronide has antinociceptive properties and has been associated with hyperalgesia and myoclonus.12,13 Morphine-6-glucuronide is a potent analgesic and may be more potent than morphine.14 Normorphine is another metabolite produced and may contribute to analgesic and toxic effects. The major hydromorphone metabolite is hydromorphone-3-glucuronide. This compound does not have analgesic properties, but is a more potent neuroexcitant than morphine-3-glucuronide.15 Oxycodone is metabolized to hydromorphone and has been suggested as a potentially safer alternative in some elderly or renally impaired patients, although there is no solid data to support this assertion.
Treatment
Treatment should proceed from conservative measures such as opioid reduction or rotation and reducing or discontinuing other sedative medications to addition of a psychostimulant if necessary. As with other opioid-induced side effects, dose reduction, drug rotation, evaluation for active metabolite retention, and reduction or elimination of other psychoactive substances have been suggested as initial treatment steps.
Dry Mouth
Scope
Dry mouth is an extremely common complication of chronic opioid administration and has been associated with severe dental problems. In one study, 84% of patients experienced this symptom either temporarily or throughout the entire study period, and reports of dry mouth were present in 65% of the assessments.16
Pathophysiology
This side effect appears to be the result of a direct action of opioids and their metabolites.16 The exact mechanism has not been described, but it is thought that this may be related to interference with nerve-mediated mechanisms and parasympathetic impulses activating glandular muscarinic or adrenergic receptors.17
Risk Factors
The risk of this side effect appears to be directly related to dose and in the case of morphine directly related to the amount of morphine-6-glucuronide.16 This symptom can be exacerbated by other compounds with anticholinergic effects.
Diagnosis
There are no specific diagnostic studies recommended for this side effect.
Prevention
There are no specific preventive measures for this side effect.
Treatment
Treatment can consist of opioid reduction or rotation, elimination of anticholinergic or anticonvulsant compounds with xerostomic effects, or symptomatic treatment by encouraging liquid intake. Symptomatic treatment such as fluid intake, artificial saliva, or encouraging the patient to use chewing gum or hard candy to promote saliva release may be helpful. In addition, agents that promote salivary excretion such as pilocarpine and bethanechol chloride have been advocated.17
Respiratory Depression
Scope
Respiratory depression is a very real concern to all physicians prescribing opioid analgesics and is potentially the most dangerous side effect. This side effect, like many others related to the administration of opioid analgesics, is of most concern during initiation of therapy, with significant dose increases, or when the potential for active metabolite accumulation is present. Tolerance to the respiratory depressant effects of opioids usually develops over the course of days to weeks. True respiratory depression is rare in patients who have been receiving opioids chronically.18 When it does occur, it is often related to a recent dose increase or conversion from one opioid to another. If the dose of opioid has been stable, an alternative explanation such as pneumonia, pulmonary embolism, cardiomyopathy, or recent coadministration of another sedating medication should be considered.19,20
The use of opioids in the treatment of those with severe pain near the end of life is often considered controversial due to the very real potential for a “double effect.” The moral doctrine of double effect is roughly defined as follows: Double effect provides that it can be morally good to shorten a patient’s life as a foreseen and accepted but unintended side effect of an action undertaken for a good reason, even if it is agreed that intentionally killing the patient or shortening the patient’s life is wrong. The use of sedation in the terminal setting to control the sometimes intense pain of dying patients may have the effect of shortening the patient’s life. This creates concern that the provision of appropriate palliative care mandates actions that may be indistinguishable from euthanasia, which is illegal in most places and morally objectionable to many. Invoking double effect addresses these worries: the intent of the physician is to control the suffering, not to shorten life. Evidence of physician intent should be found in notations on the patient’s chart and in the recorded dosages and titration of the opioid analgesics. Consequently, the action is not euthanasia but appropriate palliative care.21
Pathophysiology
High concentrations of opioid receptors are present in many supraspinal brain respiratory centers, including the nucleus solitarius, the nucleus retroambigualis, and the nucleus ambiguous.22 In addition, there are specific chemosensitive brain areas that mediate opioid-induced respiratory effects. Opioids interfere with pontine and medullary respiratory centers that regulate respiratory rhythmicity (Fig. 34-1). The µ-receptor action of opioids on respiratory centers in the brain stem produces dose-dependent depression by direct action on brain stem respiratory centers to the point of apnea with sufficient doses.
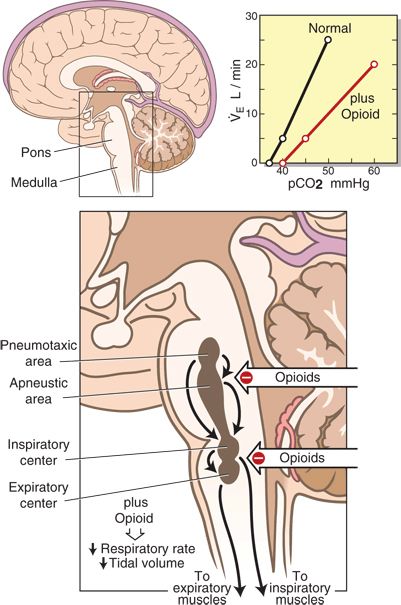
FIGURE 34-1. The pathophysiology of opioid-induced respiratory depression. Opioids bind to and inhibit respiratory centers within the medulla and pons responsible for the rate of respiration (pneumotaxic and apneustic centers) as well as the control of the muscles of inspiration and expiration that govern tidal volume. The inset is a graphic representation of the ventilatory response to progressive hypercapnia. The slope of the ventilatory response is reduced in the presence of opioids. The apneic threshold (the intercept on the x axis or the pCO2 value where apnea ensues) is shifted to the right. (Inset adapted from Bailey PL, Egan TD, Stanley TH. Intravenous opioid anesthetics. In: Miller RD, ed. Anesthesia., 5th ed. Philadelphia, PA: Churchill Livingstone, 2000:294, with permission.)
There is also controversy regarding the role of different subclasses of µ-opioid receptors in producing these effects. The exact mechanism by which the various respiratory centers involved in ventilatory drive, respiratory rhythm generation, chemoreception, and neural integration remains unclear. The net result is that the stimulatory effect of CO2 in ventilation is significantly reduced. This decreases the slopes of the ventilatory and occlusion pressure response to CO2 and minute ventilatory responses to increases of PaCO2 are shifted to the right (Fig. 34-1, inset). In addition, the resting end-tidal PCO2 and apneic thresholds are increased. Opioids also decrease hypoxic ventilatory drive.23,24 Carotid body chemoreception and hypoxic drive are blunted or eliminated by low doses of opioid analgesics. Opioids reduce the increase in respiratory drive normally associated with increased loads such as increased airway resistance.23 Opioids exert effects on control of respiratory rhythm and pattern and produce increased respiratory pauses, delays in expiration, irregular and/or periodic breathing, and decreased, normal, or increased tidal volume.25–27 The prolongation of expiratory time usually produces a greater effect on respiratory rate than on tidal volume. In most cases, although therapeutic doses may reduce respiratory rate, the resultant increase in CO2 stimulates central chemoreceptors and produces a compensatory increase in respiratory rate.
Risk Factors
Respiratory depression is a relatively rare complication in patients receiving long-term opioids. Although the role of opioids cannot be excluded in patients receiving long-term opioid therapy, alternate causes such as pneumonia, pulmonary embolism, cardiac dysfunction, or the coadministration of another sedating medication should be considered. In addition, patients with sleep apnea are at higher risk for developing altered respiratory patterns or complications related to the use of opioids.28
Diagnosis
Diagnosis of respiratory depression may be made when acquiring vital signs. However, respiratory rate is not always a reliable index of the magnitude of opioid-induced respiratory depression. High doses of opioids often eliminate spontaneous respirations, but do not necessarily produce unconsciousness. In this setting, patients may still be responsive to verbal commands and may breathe when directed to do so. Another clinical sign of opioid effect that may be observed is the presence of pupillary constriction. In the clinical setting, the most common method of evaluating respiratory depression is measuring respiratory rate and oxygen saturation while the patient is both awake and asleep. This may be accomplished with either clinical examination or electronic monitoring devices.
The use of electronic devices may provide more consistent monitoring, but alarms may be ignored. In addition, the use of monitoring such as pulse oximetry may not detect respiratory depression immediately because oxygen saturation may fall long after the beginning of respiratory depression and decreased respiratory rate. In the acute overdose situation, blood gas analysis may be required and subsequently demonstrate decreased PaO2, increased CO2, and decreased pH. In some cases, reversal of opioid effect with improvement in respiratory depression provides indirect evidence of the cause. In patients receiving chronic opioid therapy in the outpatient setting, monitoring is not employed, and mild respiratory depression may occur undetected.
Prevention
Prevention of respiratory depression is accomplished by limiting initial and total dose, avoiding situations in which significant metabolite accumulation may occur, reducing doses in patients with concurrent medications that may exacerbate respiratory depression, and adjusting doses for patients with medical conditions such as sleep apnea that increase the risk of opioid-induced respiratory depression.
Treatment
Treatment consists of opioid dose reduction, elimination or reduction of other medications with respiratory depressant or sedative effects, and in rare cases the administration of opioid antagonists. The administration of opioid antagonists should be reserved for severe respiratory depression because acute withdrawal or untoward physiologic responses to naloxone administration can occur. These include the development of increased pain, nausea, vomiting, shivering, metabolic stress, hypertension, tachycardia, pulmonary edema, cerebrovascular accident, cardiac arrhythmia, cardiac arrest, and death. In addition, due to its short half-life, if naloxone is not continued respiratory depression may recur.29–35
Hyperhidrosis
Hyperhidrosis (excessive sweating) is an adverse effect commonly reported by patients receiving oral opioids, but has received little attention in the medical literature. In one study of patients receiving methadone, the incidence of excessive sweating was 45%.36 This is thought to be related to mast cell degranulation and has been successfully controlled with antihistamines. In most cases, this is not excessively troubling to the patient and rarely requires treatment.37,38
Myoclonus
Scope
Muscular spasm (myoclonus) and tremor can occur with opioid administration. Myoclonus is often mild and self-limited, but in some cases can persist and become severe, producing distresses for both the patient and the family. Symptoms range from mild twitching to generalized spasms and can exacerbate pain due to involuntary movement. This symptom tends to occur more frequently with high doses of opioids and when patients are drowsy or entering light sleep.
Pathophysiology
The pathophysiology of myoclonus is not well characterized, but may be related to accumulation of metabolites. Following administration, opioids such as morphine and hydromorphone are metabolized primarily to morphine-3-glucuronide or hydromorphone-3-glucuronide. The 3-glucuronide metabolites are devoid of analgesic activity and have been theorized to play a role in antagonizing the antinociceptive effects of the parent compound and the active 6-glucuronide metabolite.39 It has also been implicated in potentially playing a role in the development of tolerance.
Several rodent studies have demonstrated that morphine-3-glucuronide and high-dose morphine administered by the intracerebroventricular and intrathecal routes produce symptoms of altered pain behavior such as hyperalgesia, allodynia, motor excitation, seizures, and even death.39–46 The mechanisms of these neurotoxic phenomena are not fully elucidated. There have been conflicting results in animal studies regarding the reversibility of opioid-induced neuroexcitation by naloxone, and a nonopioid receptor mechanism has been theorized.42–46 The behavioral excitation of high-dose morphine and morphine-3-glucuronide can be mimicked by the glycine antagonist strychnine.44 However, an in vitro study was unable to demonstrate inhibition of H-strychnine binding by morphine or morphine-3-glucuronide.47 Administration of N-methyl-D-aspartate (NMDA) antagonists causes a reduction of behavior excitation produced by high-dose morphine and morphine-3-glucuronide.41,48
Risk Factors
The risk of myoclonus is increased by the use of large doses of opioid analgesics and/or the accumulation of toxic metabolites and has been reported with multiple delivery routes including oral, subcutaneous, intravenous, epidural, and intrathecal. There does not seem to be a specific route of administration that is more likely to produce this side effect. The use of large doses and the accumulation of metabolites appear to play the largest role. The most common metabolites associated with this side effect are the 3-glucuronides. In addition, metabolites such as normeperidine and normorphine have been implicated.
Diagnosis
There are no specific diagnostic tests available. Although drug and metabolite levels may be obtained, levels associated with the development of symptoms in humans have not been well described. As a result, diagnosis is primarily made on the basis of history and physical examination alone.
Prevention
There are no specific preventive measures. Choosing the most appropriate compound to avoid toxic metabolite accumulation may be helpful in some cases. In other cases, switching to another opioid analgesic, opioid rotation, maximizing nonopioid analgesics, or using other interventional pain-relieving techniques may reduce the frequency and severity of symptoms.
Treatment
There are no prospective randomized trials that detail effective treatment for myoclonus. Empiric treatment usually consists of opioid dose reduction, rotation to a different opioid, or use of adjuvant analgesics. If myoclonus is persistent and other causes have been eliminated, treatment with benzodiazepines, skeletal-muscle relaxants, clonidine, acetylcholinesterase inhibitors, valproic acid, baclofen, or dantrolene has been recommended.49–60
Nausea and Vomiting
Scope
The presence of nausea and vomiting in association with opioid administration is common. Reports of the incidence of nausea in association with opioid administration range from 9% to 98%.1,18,61 Vomiting is less common and has been reported from 0% to 39%.1,18,61
Pathophysiology
Nausea and vomiting are produced by the direct effects of opioids on the chemoreceptor trigger zone in the area postrema of the medulla, possibly through the activation of δ-receptors.62 This effect, in combination with opioid-induced alterations in gastrointestinal motility, contributes to symptoms of nausea and vomiting.
Risk Factors
There are no specific risk factors for nausea and vomiting, and no specific opioid has been identified as being more emetogenic than another. These side effects, as with many others, are more common when the drug is initiated than after tolerance to the medication has developed.
Diagnosis
This diagnosis is made on the basis of history or direct observation. There are no laboratory tests to make the diagnosis of nausea.
Prevention
There is little that can be done to prevent nausea and vomiting. In some cases, one opioid may cause more nausea and vomiting for a given patient than another, and this drug should be avoided. As is commonly recommended in the treatment of chronic pain, the use of nonopioid analgesic adjuvants should be encouraged in general and as a potential means of decreasing this undesirable side effect. Avoiding opioid ingestion on an empty stomach may reduce these symptoms in some patients. There is no evidence from prospective trials to recommend the prophylactic use of antiemetics in the treatment of opioid-induced nausea and vomiting.
Treatment
Treatment of nausea may incorporate the use of a variety of compounds. However, it should be noted that recommendations for the use of these agents in the setting of chronic opioid therapy is unsupported by prospective study or systematic evaluation of retrospective data. Agents such as ondansetron, granisetron, metoclopramide, phenergan, prochlorperazine, dimenhydrate, phenothiazine, transdermal scopolamine, cisapride, and dexamethasone have all been suggested. In several case reports, the prevalence and severity of nausea and vomiting were reduced by rotation to another opioid.63–65 There are two small studies demonstrating a reduction in nausea and vomiting by converting from oral to subcutaneous administration.66,67 Data regarding the use of rectal administration is conflicting.68,69 In rare cases, the use of an opioid antagonist or discontinuation of the opioid altogether may be required to eliminate nausea and vomiting.
 ENDOCRINE EFFECTS OF CHRONIC OPIOID THERAPY
ENDOCRINE EFFECTS OF CHRONIC OPIOID THERAPY
Scope
Adverse effects of opioids on the endocrine system have been observed for almost a century, but are often not presented during medical education or in discussions with patients regarding the risk of using opioid analgesics. These complications include central hypogonadism, adrenocortical deficiency, and growth hormone deficiency (Box 34-3). Symptoms of hypogonadism include loss of libido, impotence, infertility (males and females), depression, anxiety, fatigue, loss of muscle mass and strength, amenorrhea, irregular menses, galactorrhea, osteoporosis, and fractures.70–80 Symptoms of adrenocortical deficiency include insidious onset of slowly progressive fatigability, weakness, anorexia, nausea and vomiting, weight loss, cutaneous and mucosal pigmentation, hypotension, and occasional hypoglycemia.81–83 The spectrum may vary depending on the duration and degree of adrenal hypofunction and may range from mild chronic fatigue to fulminating shock. Symptoms of growth hormone deficiency in adults are uncertain.83
BOX 34-3 Endocrine Effects of Chronic Opioid Therapy
 Central hypogonadism
Central hypogonadism
 Loss of libido
Loss of libido
 Impotence
Impotence
 Infertility (males and females)
Infertility (males and females)
 Depression
Depression
 Anxiety
Anxiety
 Fatigue
Fatigue
 Loss of muscle mass and strength
Loss of muscle mass and strength
 Amenorrhea, irregular menses
Amenorrhea, irregular menses
 Galactorrhea
Galactorrhea
 Osteoporosis and fractures
Osteoporosis and fractures
 Adrenocortical deficiency
Adrenocortical deficiency
 Insidious onset of slowly progressive fatigability
Insidious onset of slowly progressive fatigability
 Weakness
Weakness
 Anorexia
Anorexia
 Nausea and vomiting
Nausea and vomiting
 Weight loss
Weight loss
 Cutaneous and mucosal pigmentation
Cutaneous and mucosal pigmentation
 Hypotension
Hypotension
 Occasional hypoglycemia
Occasional hypoglycemia
 Growth hormone deficiency
Growth hormone deficiency
 Growth hormone deficiency in adults is of uncertain consequence
Growth hormone deficiency in adults is of uncertain consequence
Related posts:

Full access? Get Clinical Tree


