CHAPTER 106
Coccyx Fracture
(Tailbone Fracture)
Presentation
The patient slipped and fell on his buttocks or tailbone, was kicked or injured during an athletic activity, directly impacting the sacrococcygeal synchondrosis, and now complains of pain at the tip of his spine that is worse with sitting and perhaps with defecation. There should be little or no pain with standing, but walking may be uncomfortable. On physical examination, there is point tenderness and perhaps deformity of the coccyx that may be best palpated by examining through the rectum with a gloved finger (Figure 106-1).
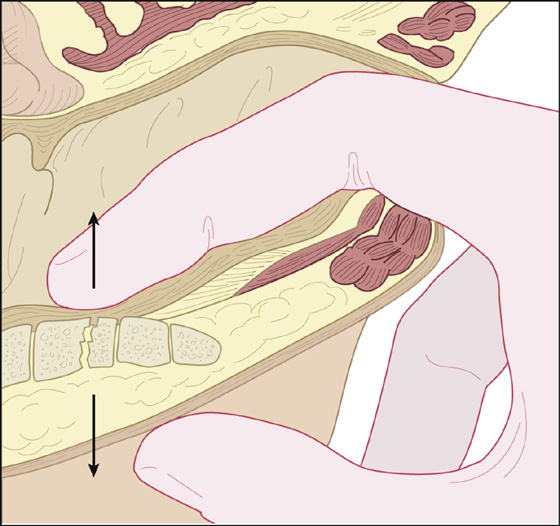
Figure 106-1 Finger palpating the coccyx by rectal examination.
What To Do:
 Verify the history (was this actually a straddle injury?) and examine thoroughly, including the lumbar spine, pelvis, and legs. Palpate the coccyx from inside and out, feeling primarily for point tenderness and/or pain on motion. Often, with gentle examination with a gloved hand, the entire coccyx can be examined and tested for stability without the discomfort of a rectal examination.
Verify the history (was this actually a straddle injury?) and examine thoroughly, including the lumbar spine, pelvis, and legs. Palpate the coccyx from inside and out, feeling primarily for point tenderness and/or pain on motion. Often, with gentle examination with a gloved hand, the entire coccyx can be examined and tested for stability without the discomfort of a rectal examination.
 Radiographs are optional and probably should be avoided. Any noticed variation can be an old fracture or an anatomic variant, and a fractured coccyx can appear within normal limits.
Radiographs are optional and probably should be avoided. Any noticed variation can be an old fracture or an anatomic variant, and a fractured coccyx can appear within normal limits.
 The diagnosis can usually be made clinically. If there is a tender deformity, especially if accompanied by movement or crepitus of the distal segment, a fracture of the coccyx is most probable. Exquisite tenderness alone is an indication of contusion or a stable nondisplaced fracture. The therapy is the same for both contusion and fracture.
The diagnosis can usually be made clinically. If there is a tender deformity, especially if accompanied by movement or crepitus of the distal segment, a fracture of the coccyx is most probable. Exquisite tenderness alone is an indication of contusion or a stable nondisplaced fracture. The therapy is the same for both contusion and fracture.
 Reassurance and an explanation of your findings and presumed diagnosis will be satisfying to most patients without having to get radiographs, especially when the patients are informed about the frequent inaccuracy of radiographs and the fact that you do not want to expose their genital area to any unnecessary irradiation.
Reassurance and an explanation of your findings and presumed diagnosis will be satisfying to most patients without having to get radiographs, especially when the patients are informed about the frequent inaccuracy of radiographs and the fact that you do not want to expose their genital area to any unnecessary irradiation.
 Instruct the patient in how to sit forward, resting his weight on ischial tuberosities and thighs, instead of on the coccyx. A foam-rubber doughnut cushion or gel cushion may help. If necessary, prescribe or recommend acetaminophen or anti-inflammatory pain medications and stool softeners. Cold packs or hot sitz-type baths may provide further comfort. Avoid narcotics when possible, because constipation may aggravate the coccygeal pain.
Instruct the patient in how to sit forward, resting his weight on ischial tuberosities and thighs, instead of on the coccyx. A foam-rubber doughnut cushion or gel cushion may help. If necessary, prescribe or recommend acetaminophen or anti-inflammatory pain medications and stool softeners. Cold packs or hot sitz-type baths may provide further comfort. Avoid narcotics when possible, because constipation may aggravate the coccygeal pain.
 Inform the patient that the pain will gradually improve over 1 to 4 weeks as bony callus forms and motion decreases, and arrange for follow-up as needed.
Inform the patient that the pain will gradually improve over 1 to 4 weeks as bony callus forms and motion decreases, and arrange for follow-up as needed.
 If pain persists for a minimum of 2 months, consider injection of corticosteroid (i.e., methylprednisolone [Depo-Medrol] 20 mg) or therapeutic ultrasound. Chronic pain is rare, but treatable, by surgically removing the coccyx.
If pain persists for a minimum of 2 months, consider injection of corticosteroid (i.e., methylprednisolone [Depo-Medrol] 20 mg) or therapeutic ultrasound. Chronic pain is rare, but treatable, by surgically removing the coccyx.
Discussion
The term coccyx actually comes from the Greek term kokkoux (for cuckoo) because it resembles the shape of a cuckoo’s beak.
A fracture, contusion, or partial dislocation of the sacrococcygeal junction can cause painful, abnormal movement of the coccyx, especially when sitting pressure is applied to this region. Resulting pain can involve use of the levator ani muscle and the anococcygeal, sacrotuberal, and sacrospinal ligaments, as well as the gluteus maximus muscles.

Full access? Get Clinical Tree


