Chapter 21 Cleaning, disinfection and sterilization
Introduction
All staff involved with anaesthetic equipment have a duty of care to ensure that the risk of hospital-acquired infection from anaesthetic equipment is kept to an absolute minimum. To this end in the UK, guidelines on infection control in anaesthesia were first published by the Association of Anaesthetists of Great Britain and Ireland (AAGBI) in 2002 and updated in 2008.1 Also in the UK, healthcare organizations now have a legal responsibility to implement changes to reduce healthcare-associated infections (HCAIs). The Health Act 20062 provided the Healthcare Commission with statutory powers to enforce compliance with the Code of Practice for the Prevention and Control of Healthcare Associated Infection.
Although there are only a limited number of published reports relating to cross-infection,3,4 the AAGBI recommendation was that all reusable anaesthetic equipment must be appropriately decontaminated prior to patient use and single-use items must be discarded immediately following use. Unfortunately, wide variation in decontamination practices between anaesthetic departments is well recognized. This can be avoided by ensuring that every hospital has a comprehensive infection control policy in place for all anaesthetic equipment, with a nominated anaesthetist and infection control doctor (ICD) taking lead responsibilities.5 Such a policy should be evidenced-based and subject to periodic audit and review. Other useful UK web-based resources include the National Resource for Infection Control and the NHS Library (Surgery, Theatres and Anaesthesia Specialist Library). Key areas requiring risk assessment are listed in Table 21.1.
The aim of this chapter is not to be prescriptive, but to provide the necessary background information for a hospital to formulate its own anaesthetic equipment infection control policy in order to minimize the risk of HCAIs and comply with the UK’s ‘Health Act 2006’.2
Risk assessment and the decontamination process
Contaminated medical devices are typically classified into three infection risk categories:6
1. High risk (critical) devices – items in contact with a break in the skin, mucous membranes or introduced into a sterile body area. Such items must be sterile at the time of use. Examples include surgical instruments, dressings, catheters and prosthetic devices.
2. Intermediate risk (semi-critical) devices – defined as devices in contact with intact mucous membranes or contaminated with readily transmissible organisms (which do not penetrate skin or enter sterile parts of the body – see high risk devices). Disinfection is required though sterilization is preferred if the devices are heat-stable. Examples include endoscopes and respiratory equipment.
3. Low risk (non-critical) devices – items in contact with healthy intact skin. Cleaning, typically using hot water and a neutral detergent or a disposable detergent wipe, and drying are adequate for such items. Examples include non-disposable ECG electrodes, sphygmomanometer cuffs and stethoscopes.
If disposable anaesthetic equipment is chosen (Fig. 21.1), then a risk assessment may not be required. However, it is important to remember that disposable equipment will be for ‘single use’ or ‘single patient use’ only. ‘Single use’ indicates that the manufacturer intends the item to be used once only on an individual patient and then discarded. The packaging will be labelled either ‘Single use’, ‘Do not re-use’ or with the symbol  .
.

’Single patient use’ indicates that the manufacturer advises that the item may be used more than once on the same patient.7 Examples of ‘single patient use’ items in anaesthesia include ventilator tubing and bacterial/viral filters used in critical care units.
Terminology
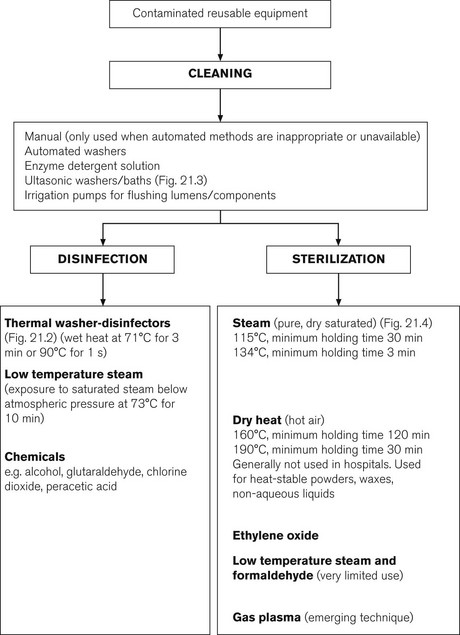
Cleaning
This is the physical removal of infectious agents or organic matter. It involves washing with a solvent (usually water and detergent), which may be heated (e.g. thermal washer disinfection, Fig. 21.2). This process does not necessarily destroy infectious agents. It is an essential process prior to disinfection or sterilization to remove bioburden. Items may also be placed in a water bath incorporating an ultrasound generator (Fig. 21.3). The ultrasound causes the water to vibrate at high frequencies so that it literally ‘shakes’ off organic matter. Ultrasonic washers are particularly useful for equipment where conventional cleaning methods might not reach some aspects of the device, or where items are too delicate to be physically scrubbed (e.g. some ophthalmic instruments).


Sterilant
This is a liquid chemical agent, which can kill bacteria, fungi, viruses and bacterial spores (e.g. gluteraldehyde, chlorine dioxide, peracetic acid). However, this term is not precise and is not generally used. The term high-level disinfectant is preferred. A flow chart of appropriate decontamination methods is shown in Fig. 21.4.