Key Clinical Questions
What conditions can mimic an acute exacerbation of chronic obstructive pulmonary disease (COPD) and require different diagnostic and treatment modalities?
What inpatient therapeutic modalities can help reduce mortality or length of stay for patients with exacerbation of COPD?
What medications should be utilized for a patient who is being discharged after an acute exacerbation of COPD to prevent further exacerbations?
What are the appropriate situations for use of noninvasive ventilation for patients with an acute exacerbation of COPD?
Other than medications, what modalities need to be considered and discussed with a patient at the time of discharge after an acute exacerbation of COPD?
Introduction
Chronic obstructive pulmonary disease (COPD) is a group of clinical and pathological pulmonary disorders that are preventable and treatable and are characterized by airflow limitation that is not fully reversible. The most common phenotypes of COPD are emphysema and chronic bronchitis. Emphysema is generally defined by pathologic and physiologic criteria as irreversible enlargement of the airways and loss of elastic recoil. Clinically, emphysema is characterized by dyspnea along with an expanded chest, decreased breath sounds, radiographic lucency, and flattening of the diaphragms. Chronic bronchitis is defined clinically by the finding of cough and sputum production on most days of at least 3 months per year for 2 consecutive years. Pathologically, the hallmark of chronic bronchitis is large airway inflammation and the hypertrophy and hyperplasia of the mucous-secreting goblet cells. The diagnosis of COPD requires spirometry which should be obtained in patients (at a time free of exacerbation) who exhibit cough, sputum production, dyspnea or risk factors/exposure history. COPD is defined clinically by airflow limitation on pulmonary function tests that is not fully reversible. The severity of COPD is classified by the degree of limitation in the forced expiratory volume in 1 second (FEV1) (Table 239-1).
| GOLD Stage | Severity | Symptoms | Spirometry |
|---|---|---|---|
| 0 | At risk | Chronic cough, sputum production | Normal |
| I | Mild | With or without chronic cough or sputum production | FEV1/FVC < 0.7 and FEV1 80% predicted |
| II | Moderate | With or without chronic cough or sputum production | FEV1/FVC < 0.7 and 50% FEV1 < 80% predicted |
| III | Severe | With or without chronic cough or sputum production | FEV1/FVC < 0.7 and 30% FEV1 < 50% predicted |
| IV | Very severe | With or without chronic cough or sputum production | FEV1/FVC < 0.7 and FEV1 < 30% predicted |
| or | |||
| FEV1 < 50% predicted with respiratory failure or signs of right heart failure |
Hospitalists often manage patients presenting with new symptoms consistent with COPD, patients with acute exacerbations of underlying COPD, and patients whose COPD complicates the course of care for other medical conditions. In this chapter, we will review best practices for each of these scenarios and solutions for optimizing care of these patients as they transition out of the acute care setting.
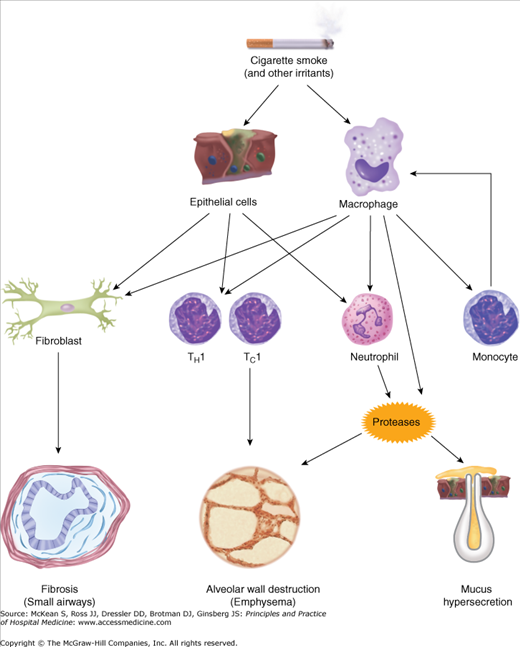
Tobacco smoking is the single most important risk factor for the development of COPD. Cigarette, pipe, and cigar smoking account for more than 90% of cases of COPD; yet, clinically important disease is only found in 10% to 20% of smokers. Clearly there are other predisposing factors because dose-dependent exposure to tobacco does not wholly determine the onset or severity of disease in COPD. Other factors that lead to the onset (or accelerate the progression) of COPD include exposure to second-hand smoke, environmental irritants and pollutants (including biomass), occupational exposures, malnutrition, early life pulmonary infections, HIV infection, and genetic predisposition. The role of genetics is incompletely understood, but COPD is more common in the relatives of those with COPD.
Tobacco smoke and other exposures cause inflammatory, biochemical and anatomic changes that account for the symptoms, limitations, and complications of COPD (Figure 239-1). Anatomically, the central airways, peripheral airways, lung parenchyma and pulmonary vasculature are all affected. Irritant exposure and yet-to-be elucidated host factors interact to result in an inflammatory process, and an imbalance of proteinases, anti-proteinases and oxidative stress. Physiologically, ciliary dysfunction, mucous hypersecretion, loss of elastic recoil, airflow limitation, impaired gas exchange and pulmonary hypertension can all be manifestations.
Epidemiology
Estimates of the rates of COPD in the United States and worldwide vary widely, but data are consistent that the disease burden is large and COPD is underdiagnosed. Survey data from 2007 estimate that 10.2 million Americans have COPD. COPD accounted for 672,000 hospital admissions in 2006 and caused 127,049 deaths in 2005, according to the American Lung Association. COPD is known to be increasing among women and is the fourth leading cause of death in both the United States and Europe.
There is increasing evidence that patients with COPD have high rates of morbidity and mortality caused by extrapulmonary problems. Patients with COPD have been found to have higher rates of cardiovascular, gastrointestinal and psychiatric illnesses among others. It is estimated that COPD is a primary or contributing cause of almost 10% of all admissions to the hospital. Cardiovascular morbidity and mortality might be even higher than that of lung disease and respiratory failure.
COPD Exacerbation: Differential and Evaluation
An acute exacerbation of COPD (AECOPD) is defined as a change in the baseline symptoms of dyspnea, cough and/or sputum color or volume that necessitates a change in management. When a patient with COPD or risk factors for COPD presents with any of these complaints, the diagnosis of AECOPD must be considered against a number of other diagnoses that can mimic an AECOPD. Once a diagnosis of AECOPD is reached, issues of causation of the exacerbation and level of severity need to be addressed. There is no single agreed-upon system to rank severity of exacerbations, but broadly categorizing among three levels has been suggested: (1) home management; (2) hospital management; and (3) respiratory failure.
AECOPD has many different potential causes and the specific trigger for any one event is sometimes never elucidated. It is commonly agreed, however, that various triggers cause acute inflammation superimposed on the chronic inflammation of the underlying disease. During an AECOPD, inflammatory cells of many inflammatory pathways can be found in sputum and blood. Together, all infectious agents (bacteria, virus, and other) account for up to 80% of acute exacerbations.
The differential diagnoses to consider as triggers in patients that have underlying COPD and an acute respiratory decompensation is extensive (Table 239-2). Many of these triggers incite the inflammatory pathway at the root of an AECOPD, but they may also require other specific therapy. When a trigger is not immediately obvious from history and physical exam, there are certain other diagnoses that must be considered. A recent autopsy study of patients that were diagnosed as having an AECOPD and that died within 24 hours of admission showed that 37% of these deaths were due to heart failure and 21% due to pulmonary embolism. Patients admitted with otherwise unexplained exacerbations of COPD are often found to have pulmonary emboli when this diagnosis is pursued.
|
Diagnostic Evaluation
For patients with known or suspected COPD, any complaint consistent with a COPD exacerbation warrants a thorough investigation. The degree of diagnostic evaluation should be determined by the patient’s subjective degree of discomfort, physical exam abnormalities and/or any alterations in vital signs or diagnostic studies. Careful consideration of any conditions in the differential diagnosis of AECOPD (Table 239-2) must be undertaken.
Along with questions regarding a change in dyspnea, a new or changed cough, and a change in sputum color and volume, the history helps establish the change from the patient’s baseline symptoms. The history may also provide clues to other diagnoses or triggers (Table 239-2) for patients suspected of having an AECOPD.
For patients with suspected AECOPD, but without a diagnosis of COPD, questioning regarding age, smoking status, exercise tolerance and other respiratory exposures can help increase or decrease the suspicion of COPD as the underlying disease.
AECOPD is associated with increased dyspnea, increased sputum purulence, wheezing, constitutional symptoms (fever, malaise, myalgias, etc), and cough. Other past medical history and comorbid conditions can affect overall mortality and may influence patient triage for monitoring and therapy.
The physical exam can help identify undiagnosed COPD, exclude other diagnoses in the respiratory decompensation of patients with known COPD, and help triage the severity of a diagnosed AECOPD. For evaluating the severity of an exacerbation, ominous physical exam findings portending higher risk and poorer outcomes include altered mentation (agitation and/or obtundation), respiratory muscle retraction, paradoxical abdominal movement, cyanosis and diaphoresis. These findings necessitate higher levels of monitoring and expedited care. Other findings that are consistent with an AECOPD include wheezing, cough, hyperresonance, expanded lung fields on lung percussion and diffusely decreased breath sounds.
In the initial evaluation of AECOPD, pulse oximetry O2 saturation > 89% is evidence of acceptable oxygenation.
|
Arterial blood gases (ABGs) are able to more accurately determine the derangement of gas exchange by calculating an alveolar-arterial gradient, and may detect worse hypoxia than expected or evidence of hypercarbia. Importantly, the pH from the ABG may also provide valuable information helping direct management (eg, consideration of noninvasive ventilation). Arterial blood gas interpretation must take into account the patient’s baseline status. Patients with more severe disease are likely to have elevated partial pressure of carbon dioxide (Pco2) with a relatively preserved pH as the kidneys compensate for chronic hypoventilation. Ominous findings include elevated Pco2 with a decreased pH (indicating an acute onset or worsening of hypoventilation), low partial pressures of oxygen, and severely elevated Pco2.
Guidelines recommend hematology profiles and basic chemistry panels in the evaluation of COPD. These tests may show polycythemia associated with chronic COPD, or conversely, anemia. These basic labs are most valuable in identifying other diagnoses to be considered or comorbid conditions that may require parallel treatment. If patients are known or suspected to be treated with theophylline, the serum levels of the drug should be measured.
Routine collection of sputum for gram stain and culture is not recommended in the management of COPD exacerbation. Sputum gram stain and culture may play a role in the laboratory evaluation of patients that do not respond to initial therapy and/or have evidence of frank pneumonia.
Chest radiography is indicated for evaluation of AECOPD. Findings on the radiograph may influence the type of care if there are findings such as pneumothorax, atelectasis, focal infiltrate or pulmonary edema. About 20% of patients thought to have an AECOPD have chest radiograph findings that influence management.
|
Patients with dyspnea and other chest complaints need electrocardiography (ECG) evaluation to identify relevant findings including coronary ischemia or arrhythmias. The irregular rhythm of multifocal tachycardia (MAT) that is found frequently in COPD patients may be difficult to distinguish from atrial fibrillation without the ECG. MAT responds to the treatment of the underlying lung disease and rate control whereas atrial fibrillation requires additional therapeutic approaches.
Triage: Determining Severity, Indications for Admission, and Level of Care
No single system exists to classify patient severity of illness once they are identified as having an AECOPD. The American Thoracic Society and European Respiratory Society (ATS/ERS) guidelines define severity based upon where the exacerbation is managed (home versus inpatient versus ICU) requiring clinicians evaluating patients for AECOPD to rely on previously mentioned risk factors for mortality and clinical acumen to best triage patients.
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) and ATS/ERS guidelines for management of COPD provide criteria for hospitalization in AECOPD (Table 239-3). Numerous studies have tried to identify patient characteristics that successfully predict patient prognosis and lower risk patients who could be managed as outpatients, but no prediction rules have been successful. Certain findings may predict the success or failure of outpatient management. Older age, lower baseline FEV1, hypoxemia, previous recent exacerbations and extensive comorbidities can increase risk of mortality or relapse exacerbation.
|
The best location to manage any particular patient with an AECOPD will vary based on individual hospital resources and staffing, with differences in the availability of specified inpatient respiratory units, step-down or intermediate care units and personnel. Therefore, criteria for intensive care unit (ICU) admission or monitoring is often institution specific. Nonetheless, some guidelines suggest criteria for ICU admission (Table 239-4).
Related posts:
 Strategies for Cost-Effective Care
Strategies for Cost-Effective Care
 Building, Growing, and Managing a Hospitalist Practice
Building, Growing, and Managing a Hospitalist Practice
 Designing a Hospitalist Compensation and Bonus Plan
The Face of Health Care Emerging Issues for Hospitalists
Designing a Hospitalist Compensation and Bonus Plan
The Face of Health Care Emerging Issues for Hospitalists
 Medical Malpractice
Preventing and Managing Adverse Patient Events: Patient Safety and the Hospitalist
Medical Malpractice
Preventing and Managing Adverse Patient Events: Patient Safety and the Hospitalist

Full access? Get Clinical Tree


