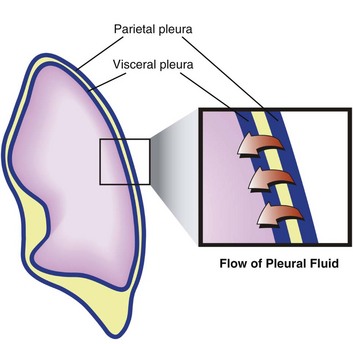
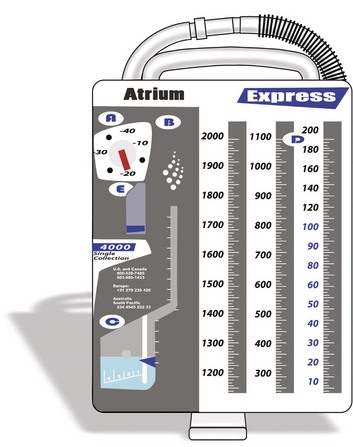
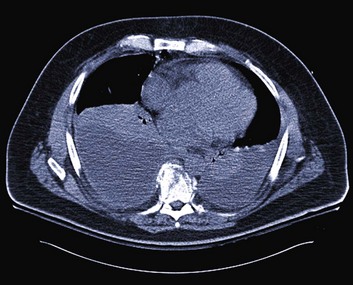
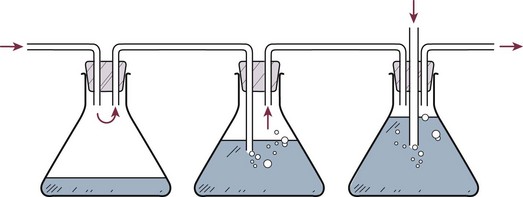
15 Hippocrates drained an empyema using a metal tube.1 Playfair developed underwater seal drainage of chest tubes in 1875.2 Credit for the invention of the chest tube is usually given to Hewett,3 who in 1876 devised a system of continuous drainage of the empyema cavity using a rubber catheter that drained into a glass jar filled with a weakly antiseptic solution.4 Use of the chest tube was not widely adopted, however, until the 1917 influenza epidemic.5 Closed tube thoracostomy drainage of the pleural space after thoracotomy was first reported by Lilienthal in 1922.6 The pleural space is the interface between the chest wall and the lung and represents a critical component of pulmonary function. The visceral and parietal pleurae are composed of a single layer of mesothelium. The blood supply of the parietal pleura is of systemic origin (intercostal vessels), whereas the blood supply of the visceral pleura is of pulmonary origin (pulmonary artery and veins). The bronchial arteries may contribute significantly to the blood supply of the visceral surface.7 Pleural fluid may originate from three sources—parietal capillaries, visceral capillaries, or interstitium. Starling’s law of transcapillary exchange governs the movement of fluid across the pleural space. The pressure in the capillaries of the visceral pleura is less than that in the parietal capillaries because it drains into the pulmonary venous bed. The net hydrostatic pressure (35 cm H2O) favors movement of fluid from the parietal pleura to the pleural space (Fig. 15.1). This pressure is derived from the subtraction of −5 cm H2O (pleural pressure) from 30 cm H2O (parietal hydrostatic pressure). This net hydrostatic pressure is opposed by the net oncotic pressure (29 cm H2O), which is derived from the subtraction of 5 cm H2O (pleural oncotic pressure) from 34 cm H2O (plasma oncotic pressure). A gradient of 6 cm H2O (34 − 29 cm H2O) favors pleural fluid formation.8 The pleural lymphatics prevent the accumulation of this pleural fluid. Stomas, unique to the parietal pleura, facilitate communication between the pleural space and the capillaries. It is estimated that this mechanism allows clearance of 20 mL of pleural fluid per hour per hemithorax in a 70-kg human.9,10 The lymphatic network clears protein from the pleural space; smaller molecules can be directly absorbed by the pleural capillaries. Intercostal and diaphragmatic muscle activity influences the rate of lymphatic flow. Hypoventilation and anesthesia reduce lymphatic flow and the rate of absorption of protein.11 The original three-bottle system has been compartmentalized into a plastic unit that is easily transportable and readily pressure-adjustable, consisting of a trap bottle, a water-seal bottle, and a manometer bottle (Fig. 15.2). The trap bottle collects the pleural fluid. The water-seal bottle prevents air from returning to the pleural space during the negative pleural pressure phase on inspiration. The manometer bottle uses the distance below its fluid line to generate a negative pressure when suction is applied. For example, 20 cm of water generates a −20 cm H2O pressure.12 Modern collection and suction systems use a single compartmentalized system (Fig. 15.3). Figure 15.2 Three-bottle system consisting of (from left to right) trap bottle, water-seal bottle, and manometer bottle. Pneumothorax is defined as air that has entered the pleural space, either spontaneously or as a result of traumatic tears in the pleura after chest injury or after invasive procedures. Treatment of pneumothorax entails removing air from the pleural space, reexpanding the underlying lung, and preventing recurrence.13 If the patient is clinically stable, the treatment depends on the size of the pneumothorax and whether or not the patient is mechanically ventilated. If the pneumothorax is small, and the patient is not mechanically ventilated, the pneumothorax can be observed. If the pneumothorax is large, or the patient is mechanically ventilated, a chest tube should be placed.14 A large pneumothorax is defined as being greater than 15% to 20%.15 Needle aspiration has also been described as a consideration for treatment of spontaneous pneumothorax. However, a repeat chest radiograph must be obtained to assure no recurrence in which case a chest tube would be required.16 If an occult pneumothorax is identified, which is a pneumothorax found incidentally on computed tomography (CT) scan without evidence clinically or on chest radiograph, observation may be an option. The optimal management remains controversial with regard to tube placement; however, two retrospective reviews demonstrate safe observation without tube placement in patients requiring positive-pressure ventilation.17,18 Tension pneumothorax is a life-threatening clinical situation that requires emergent and immediate treatment (Fig. 15.4). Air collects and builds up pressure in the chest cavity through a tear in the lung or bronchial tree. Air enters the chest with each mechanical or spontaneous breath, with no route for escape. Initially, the affected lung simply collapses, but as tension increases, the diaphragm flattens, and the mediastinum is shifted toward the contralateral side.19 The contralateral lung is compressed, further decreasing effective ventilation. The great vessels also are compressed, and venous return is reduced drastically. This reduction in venous return results in rapid and disastrous cardiopulmonary collapse.20 The diagnosis is ideally made on a clinical basis, and treatment is initiated without waiting for radiographic confirmation. Any tension pneumothorax should have immediate large-bore needle decompression. A readily available large-bore angiocatheter is preferentially inserted in the second intercostal space at the midclavicular line. A rush of pleural air under pressure confirms the diagnosis and location. After decompression (conversion to a simple pneumothorax), the catheter is left in until a tube thoracostomy has been placed.21 Pleural effusions, both transudative and exudative, are frequently seen in the ICU. The incidence of pleural effusions in the ICU varies with screening methods, from approximately 8% for physical examination to more than 60% for routine ultrasound.22,23 Several factors contribute to the occurrence of pleural effusions in ICU patients. Large amounts of intravenous fluid are often administered during the first few days to patients admitted for shock. Pneumonia also is common as a reason for ICU admission and as a complication of mechanical ventilation. Heart failure, atelectasis, hypoalbuminemia, and liver disease are present in many ICU patients. In surgical ICUs, cardiac or abdominal surgery is often followed by specific, large, protracted pleural effusion; in multiple-injury patients, hemothorax is possible.24 The criteria of Light and colleagues,25 which are based on the ratio of protein or lactate dehydrogenase levels in the pleural fluid and blood, differentiate exudates from transudates with a negative predictive value of 96% and a sensitivity of 98%.24 Provided that basic rules are followed, thoracentesis is safe in ICU patients.22 A chest tube may be placed for large or symptomatic pleural effusions. The optimal drainage duration for uninfected pleural effusions has not been established. A reasonable approach may be to remove the chest tubes when drainage decreases to less than 200 mL/day.26 In the evaluation of a parapneumonic effusion or empyema, if the thickness of the pleural fluid is more than 10 mm on a decubitus radiograph, or if the pleural fluid is of similar depth and loculated, the pleural fluid should be examined to determine the stage of the effusion. Drainage of an infected pleural space is required to achieve source control as a key component of treatment (Fig. 15.5). If the fluid is removed completely and does not reaccumulate, no additional therapy need be directed toward the effusion. At the time of the initial therapeutic thoracentesis, the pleural fluid should be sent for Gram stain and culture and analysis of leukocyte, lactate dehydrogenase, glucose, and pH levels. Indicators of a poor prognosis from the pleural fluid include positive Gram stain or culture, glucose less than 60 mg/dL, lactate dehydrogenase more than three times the upper limits of normal for serum, or pH less than 7.20. If the therapeutic thoracentesis removes all of the pleural fluid and the fluid recurs, the next step is guided by the initial pleural fluid findings. If none of the poor prognostic indicators is present, no invasive procedures are indicated if the patient is doing well clinically. If any of the poor prognostic indicators were present at the initial thoracentesis, a second therapeutic thoracentesis should be performed, and the pleural fluid should be reanalyzed. If the pleural fluid accumulates a third time, a small chest tube should be inserted into the pleural space, unless none of the poor prognostic factors were present at the time of the second thoracentesis.27 If the patient shows signs of systemic infection, and fluids have been inadequately drained, an open thoracotomy and drainage may be required.28,29 When a hemothorax is suspected, the essential management, along with appropriate resuscitation, is intercostal drainage. This achieves two objectives: first, to drain the pleural space, allowing expansion of the lung, and second, to allow assessment of rates of continuing blood loss. After satisfactory resolution of hemothorax managed with intercostal drainage alone, the drain should not be removed too promptly. Other circumstances permitting, the patient should be mobilized fully with adequate thoracic physiotherapy. These measures should allow optimal drainage of the pleural cavity.30 Complete drainage of blood also prevents empyema and fibrothorax.31 Pneumomediastinum is usually a self-limited entity (Fig. 15.6). It follows alveolar rupture into the pulmonary interstitium and is produced by an acute episode of high intrathoracic pressure. The differential diagnosis includes cardiac, pulmonary, musculoskeletal, and esophageal causes. Spontaneous pneumomediastinum is usually a self-limited clinical entity.32 Coupled with positive-pressure ventilation or subcutaneous emphysema, however, cautious observation is recommended owing to the possibility of a pneumothorax leading to tension pneumothorax. Figure 15.6 Pneumomediastinum (arrow). The pneumomediastinum occurred during a forceful singing period. If the diameter of the tube is doubled, flow increases by a factor of 16, implying that a small increase in the size of the drainage tubes would result in substantial improvements in the flow rates.33 where v is the flow, r is the radius, l is the length, P is the pressure, and f is the friction factor.12,34–36 In an in vitro study, Park and coworkers37 measured flow rates of different viscosity fluids (serous, blood, pus) through catheters of different diameters, ranging from 6F to 18F, and found that flow rates increased for larger catheters as predicted by Poiseuille’s law. At catheter sizes larger than 7F, however, the differences were small. Reports on drainage techniques suggest that before drainage of a collection, diagnostic needle aspiration should be performed, initially with a 22-gauge needle and, if this is unsuccessful, subsequently with a 20-gauge or 18-gauge cannula.38 It has been postulated that if pus can be aspirated by such a needle, it should be drainable through a catheter twice the size (i.e., >6F).39 As such, if drain patency can be maintained, the maximum flow rate of the catheter is unlikely to be the limiting factor for most pleural collections.33 Given the variety of liquids and accompanying pleural debris that may be drained by a chest tube, no single formula exists for flow of these many materials. The principal determinants of airflow through a tube, bore and length, are logically key determinants of flow for various pleural liquids, including blood and pus. Chest tube selection must take into account not only what material is being drained but also its rate of formation. Ongoing production of more viscous fluids requires a larger bore tube than for a similar volume of air produced.40
Chest Tube Thoracostomy
History
Anatomy and Physiology of the Pleural Space
Drainage Systems
Indications and Contraindications
Simple Pneumothorax
Tension Pneumothorax
Pleural Effusions

Chest Tube Size

Related posts:

Full access? Get Clinical Tree


Anesthesia Key
Fastest Anesthesia & Intensive Care & Emergency Medicine Insight Engine