Chapter 3 Chest pain
Introduction
Chest pain is the commonest reason for 999 calls and accounts for 2.5% of out-of-hours calls. Of patients taken to hospital, about 10% will have an acute myocardial infarction (AMI). Evidence suggests that up to 7.5% of these will be missed on first presentation. There are a number of other life threatening conditions which can present as chest pain and must not be overlooked. The objectives of this article are therefore to provide a safe and comprehensive system of dealing with this presenting complaint (Box 3.1).






Primary survey
Follow the ABC principles (Box 3.2).






Patients with normal primary survey with obvious need for hospital admission
There are three immediately life threatening medical conditions that can present with chest pain:



Fifty percent of sudden cardiac deaths occur within 1 hour of the start of a myocardial infarction and 75% within 3 hours. The benefits of thrombolysis or percutaneous intervention (PCI) are directly related to the length of time between the onset of symptoms and its delivery. Therefore if you diagnose a myocardial infarction, ensure you have immediate access to a defibrillator and consider thrombolysis or arrange rapid transportation to a facility where thrombolysis or PCI can be delivered.
Secondary survey (including history taking)
Take a history of the presenting complaint, gather relevant information, and perform an examination (see Chapter 2).
The OPQRST of chest pain
Chest pain is often categorised into three main types (Table 3.1). It can be very difficult to place any particular patient into one of these categories, but there is evidence that the characteristics of pain can help in the diagnosis:



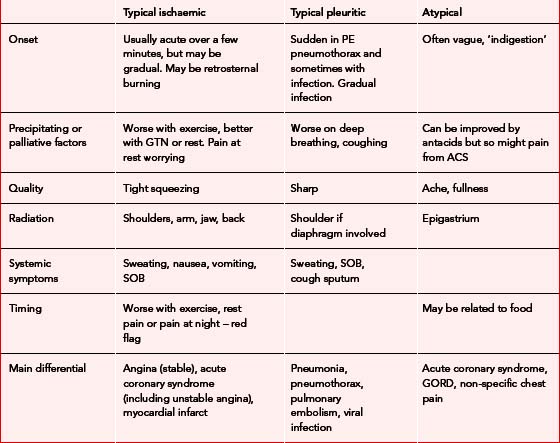
Onset of pain
The pain of a myocardial infarction is classically described as rapidly increasing over a few minutes but it can develop gradually or even be intermittent. In an acute coronary syndrome the pain may well be intermittent. As the platelet thrombus breaks down, blood flow is restored and the pain is relieved. Beware of pain starting at rest, or that which wakes the patient up from sleep.
Precipitating factors/palliative factors
Gain a detailed impression of how the pain started. Establish if there is any relation to exercise, breathing or food. Pain that has been provoked by exercise or wakened the patient should be regarded as significant. GTN will improve angina pain but also will improve pain from oesophageal problems. Equally there is no evidence that improvement of pain after giving an antacid can help distinguish between cardiac and oesophageal pain.
Other factors
Risk factors
The presence of risk factors for cardiovascular disease should increase your suspicion as to a cardiac cause for the pain (Box 3.3).






Medical history/drugs allergies
Related posts:
 Childhood illness – assessment and management of primary survey negative children
Childhood illness – assessment and management of primary survey negative children

Full access? Get Clinical Tree


