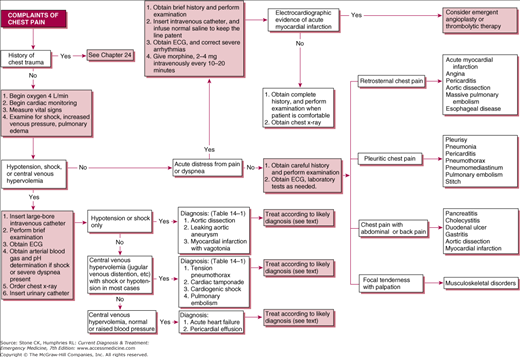
Immediate Management of Life-Threatening Problems
Give oxygen by nasal cannula or face mask, pending further evaluation.
Begin cardiac monitoring with pulse oximetry and treat life-threatening arrhythmias (Chapters 9 and 34).
Look for signs of shock. Altered sensorium, pale clammy skin, oliguria, and respiratory distress may result from arterial hypotension and poor peripheral perfusion.
Insert two large-bore (≥16-gauge) intravenous catheters. Intraosseous (IO) access is acceptable and compatible with all resuscitation infusions including thrombolytics. Obtain blood for a complete blood count (CBC), markers of cardiac injury, and basic metabolic panel (electrolytes, glucose, renal function). Begin administration of intravenous fluids based on estimate of intravascular fluid volume.
Infuse 250–500 mL of intravenous crystalloid solutions (normal saline or lactated Ringer’s). Monitor the response (blood pressure, urine output, sensorium).
Pending more precise diagnosis, infuse normal saline to keep the intravenous catheter patent or place a saline lock IV.
Briefly examine the pulmonary and cardiovascular systems, and palpate the abdomen for presence of a pulsatile mass. Obtain a 12-lead electrocardiogram (ECG). Obtain arterial blood for blood gas and pH determinations. Avoid unnecessary arterial punctures if the patient is a candidate for thrombolytic therapy for acute myocardial infarction. Obtain a portable chest radiograph. Insert a urinary catheter.
Hypovolemia is manifested by collapsed neck veins, clear lung fields on physical examination or chest X-ray, and absence of peripheral edema. Table 14–1 lists the differentiating features of the three most important conditions causing chest pain with hypotension with central venous hypovolemia.
| Findings | ||||
|---|---|---|---|---|
| Diagnosis | History | Examination | ECG | X-Rays |
| Myocardial infarction with vagotonia | Crushing chest pain; nausea | Bradycardia; stable hypotension | Acute infarction pattern and bradycardia | Nonspecific |
| Aortic dissection | Tearing chest pain; back pain; often history of hypertension | Tachycardia; pulse deficits; progressive hypotension | Nonspecific or may show ischemia or infarction pattern, left ventricular hypertrophy | Widened mediastinum; pleural fluid. CT scan is more sensitive than X-ray |
| Leaking upper abdominal aortic aneurysm | Chest and epigastric pain | Tachycardia; pulsatile epigastric mass | Nonspecific | CT scan or ultrasound is more sensitive than X-rays |
If the diagnosis is uncertain, treatment should be oriented primarily toward aortic dissection (Chapter 40). Type and crossmatch for 6–10 units of packed red blood cells. Expand intravascular volume with administration of intravenous crystalloid solution. Consider inserting a central venous catheter. For severe hypovolemia with shock, up to 3 L of crystalloid solution may be given rapidly (over 30–60 minutes) to restore normal hemodynamics until crossmatched blood is available. If there is no response to crystalloid solution, type-specific or universal donor blood (O negative, low antibody titer, or erythrocyte antigens) may be used pending the availability of crossmatched blood. Maintain blood pressure with continued infusion of blood and crystalloid solution. Obtain emergency vascular or thoracic surgical consultation.
Pulse deficits, an abdominal mass, or occult hematuria indicate aortic aneurysm or dissection. Obtain a portable chest X-ray and if the patient is stable consider computed tomography (CT) scan of the chest or abdomen and pelvis if indicated. Bedside ultrasound, if available, can be of great assistance in the diagnosis and management of these patients.
Management of thoracic aortic dissection consists of β-blockade (esmolol) to maintain heart rate less than 60–80 beats/min and vasodilators (nitroprusside) to maintain a systolic blood pressure less than 120 mm Hg, establishing the β-blockade first. Dissections involving the ascending aorta are managed surgically, while those not involving the ascending aorta are generally managed medically. For medical management, hospitalize the patient in an intensive care setting immediately for further evaluation and treatment.
Superficial veins (especially neck veins) are distended; pulmonary and peripheral edema may be present. See Table 14–2 for guidelines to differential diagnosis.
| Diagnosis | Helpful Distinguishing Features |
|---|---|
| Tension pneumothorax | Hyperresonant hemithorax with decreased breath sounds; chest X-rays diagnostic, trachea deviates away from affected side |
| Cardiac tamponade | Faint heart sounds; ECG with diffuse low voltage or electrical alternans. Pulmonary edema rare. Echocardiography diagnostic |
| Cardiogenic shock (arrhythmogenic) | ECG or cardiac monitor shows severe bradycardia or tachycardia (ventricular rate <50 beats/min, usually <40 beats/min, usually >180 beats/min). Signs of myocardial ischemia may also be present |
| Cardiogenic shock (myocardial) | Pulmonary edema almost always present. ECG almost always shows pattern diagnostic of infarction |
| Pulmonary embolism (massive) | Physical examination, ECG, and chest X-ray show signs of right heart strain. Chest X-ray may show infiltrates, effusion, or truncation of pulmonary vasculature. Confirm diagnosis by ventilation–perfusion scanning, spiral CT scan of chest or pulmonary arteriography |
(See Chapter 24) Consider tension pneumothorax immediately because this condition may be quickly and reliably differentiated from the others and is easy to treat. Look for marked respiratory distress, tracheal deviation away from the affected side, and a hyperresonant hemithorax with markedly decreased or absent breath sounds on the affected side. Chest X-ray confirms the diagnosis, but treatment should not be delayed to obtain a chest X-ray. Treatment consists of the insertion of a thoracostomy tube if one is readily available (Chapter 7). Otherwise, a 14-gauge needle inserted in the second intercostal space at the midclavicular line or in the fourth intercostal space at the anterior axillary line relieves tension in the chest until a thoracostomy tube can be inserted. Hospitalize the patient for further care.
(See Chapter 24) Cardiac tamponade should also be diagnosed early because treatment is reasonably effective but differs markedly from that for cardiogenic shock, heart failure, or pulmonary embolism. Look for hypotension, jugular venous distension, and muffled heart sounds (Beck triad). Electrocardiographic manifestations may include low voltage on all leads, electrical alternans, or diffuse ST-segment elevation typical of pericarditis. A narrow pulse pressure and pulsus paradoxus may also be present. Pulmonary edema is rare. Because acute tamponade does not cause cardiomegaly, chest X-ray is not helpful. Definitive diagnosis by noninvasive methods is best done by bedside emergency ultrasound or formal echocardiography. Attempt volume expansion with intravenous administration of 500–1000 mL of crystalloid solution over 20–30 minutes if the diagnosis is confirmed (this therapy is disastrous for cardiogenic shock). If the initial trial succeeds in elevating the blood pressure, volume expansion may be repeated once in a patient whose systolic blood pressure subsequently drops to less than 90 mm Hg.
Obtain emergency cardiothoracic consultation for therapeutic pericardiocentesis, which should be performed in the operating room or under echocardiographic or fluoroscopic guidance. If rapid, progressive hypotension develops and the patient fails to respond to volume expansion perform immediate pericardiocentesis (under ultrasound guidance if available) (Chapter 6). Hospitalize the patient at once in an intensive care unit.
See Chapter 35 for further details on the diagnosis and treatment of cardiac arrhythmias.
Give atropine, 0.5 mg intravenously; if necessary, repeat every 5–10 minutes up to a total dose of 0.04 mg/kg. An external transcutaneous pacemaker (Chapter 7) may be applied to increase the heart rate until a percutaneous transvenous pacemaker can be inserted, if indicated. Epinephrine infusion can be used for patients that do not respond to atropine. Begin an infusion at 2–10 μg/min and titrate to patient response. Assess intravascular volume and support as needed. Dopamine can be used to support blood pressure and increase myocardial contractility. Infuse at a rate of 10–20 μg/kg/min by continuous intravenous infusion. It may be administered with epinephrine or administered alone. Titrate the dose to patient response. Consider IV glucagon, 3 mg initially, followed by infusion at 3 mg/hour for patients with hypotension and bradycardia from either B-blocker or calcium channel blocker overdose.
Immediate cardioversion is the treatment of choice for tachydysrhythmia-induced shock. Deliver 50–100 J of synchronized direct current counter shock initially, and increase the shock by 50–100 J increments if there is no response. (If the patient is STABLE ie, no alteration in mental status, no chest pain, no shock or hypotension see Chapter 34).
(See also Chapter 34) In patients with no evidence of pulmonary edema, ensure adequate intravascular volume; give intravenous crystalloid solution, 250–500 mL over 30 minutes. If blood pressure improves, maintain the infusion at a rate of 100–200 mL/h. Avoid unnecessary arterial punctures in patients who may be candidates for thrombolytic therapy.
Give dobutamine 5–20 mcg/kg/min IV continuous infusion, dopamine 5–20 mcg/kg/min IV continuous infusion; increase by 1–4 mcg/kg/min q10–q30 minutes to optimal response, or a combination of both if no change in blood pressure occurs or if severe shock or pulmonary edema is present initially. Dobutamine is the drug of choice for treatment of cardiogenic shock due to pump failure. Caution: Observe for signs of dysrhythmia.
Give morphine, 2–4 mg intravenously every 5–20 minutes, until pain and dyspnea are controlled. If hypotension is a concern, then fentanyl may be used for pain. Carefully monitor the patient’s respiratory status.
Nitroglycerin should generally be avoided in patients in cardiogenic shock or blood pressure less than 90 mm Hg systolic.
Consider aspirin 325 mg orally if aortic dissection is unlikely. In patients with aspirin allergy or expected deferred catheterization clopidogrel may be used.
Obtain cardiology consultation immediately if an acute infarction pattern is evident on the 12-lead ECG. Emergency reperfusion therapy with thrombolytic agents or percutaneous coronary intervention has been shown to be of benefit in decreasing the mortality rate and the size of the infarct. If thrombolytic therapy is to be used (Chapter 35), it should be initiated in the emergency department by the emergency physician, avoiding the delay necessitated by obtaining cardiologic consultation or transporting the patient to the coronary care unit. Hospitalize the patient immediately in a coronary care or intensive care unit.
(See Chapter 33) Because massive pulmonary embolism is a difficult diagnosis to confirm rapidly, every attempt should be made to exclude other causes of chest pain with shock. Consider an emergency echocardiogram if available. Findings consistent with massive pulmonary embolism include right ventricular hypokinesis and dilation. Right ventricular dysfunction from pulmonary embolism predicts increased mortality and the need for thrombolytic therapy.
Administer 250–500 mL of normal saline over 20–30 minutes in an effort to elevate systolic blood pressure. The dose may be repeated if the trial is successful and if heart failure does not develop. In the rare patient with hypotension without central venous hypervolemia, a fluid challenge should also be given, but a larger dose (500–1000 mL of normal saline instead of 300–500 mL) may be administered.
Give dopamine (see above). If clinical signs strongly suggest pulmonary embolism and thoracic dissection has been ruled out (computerized tomography may be useful in definitively establishing either of these diagnoses), begin heparin (unfractionated or a low-molecular-weight heparin) (see Pulmonary Embolism, below, and Chapters 33 and 34). Obtain pulmonary consultation, and consider thrombolytic therapy.
Superficial veins (especially neck veins) are distended. Pulmonary and peripheral edema is common. Blood pressure is normal or (more commonly) elevated.
Acute exacerbation of congestive heart failure is the most common cause. It occasionally results from acute myocardial infarction (acute cardiogenic pulmonary edema), and less commonly from acute myocarditis or pericardial effusion.
Nitroglycerin may be quickly administered either sublingually (0.4 mg) or transdermally (nitroglycerin ointment 1.25–2.5 cm) (½–1 inch). An intravenous nitroglycerin infusion may be started in the emergency department. Monitor the blood pressure closely, and if hypotension develops, place the patient in the Trendelenburg position and decrease the infusion rate. Avoid nitrates in patients taking any selective phosphodiesterase 5 inhibitor (sildenafil [Viagra], tadalafil [Cialis], or vardenafil [Levitra]).
Give furosemide, 0.5–1.0 mg/kg, by bolus intravenous injection. The initial effect of rapid preload reduction is of immediate benefit; diuresis occurs later.
Give morphine, 2–4 mg intravenous, and repeat every 5–10 minutes until pain and dyspnea are relieved.
Give aspirin, 160–325 mg chewed, if not contraindicated. If the patient has an allergy to aspirin, use clopidogrel, 75 mg orally.
Captopril and enalapril are associated with reduced admission rates to the intensive care unit and decreased endotracheal intubation rates. Acutely, reduction in preload and afterload has been reported. For oral or sublingual captopril, a one-time dose of 12.5 or 25 mg is given; enalapril is given as a 1.25 mg intravenous infusion over 5 minutes. Avoid using ACE inhibitors in patients who are hypotensive, pregnant, hyperkalemic, or have renal insuffiency.
If the patient continues to deteriorate, consider early noninvasive positive pressure ventilation (BiPAP or CPAP); this approach may even prevent the need for endotracheal intubation.
Short-term inotropic therapy can improve hemodynamic parameters. These agents may be beneficial for patients who are unable to receive conventional therapy. Milrinone or dobutamine are reasonable choices.
Has been shown by meta-analysis to actually increase mortality but can be considered in patients who cannot tolerate nitroglyerin. It is costly and has no additive benefit to nitroglycerin.
Hospitalize the patient immediately in an intensive care setting.
The patient is in acute distress because of chest pain but is neither hypotensive nor in shock.
Evaluation of patients who complain of chest pain but are not in severe distress should proceed in a systematic fashion. The single most useful means of evaluation is the carefully elicited history supplemented by examination of the heart, lungs, abdomen, and peripheral vessels in conjunction with electrocardiography and chest X-ray. Consider most of the diagnostic possibilities at least briefly in every patient who presents with chest pain (Table 14–3).
| History | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Pain | |||||||||
| Cause | Previous Attacks of Similar Pain | Location | Character | Onset | Duration | Common Associated Findings | Signs | Other Abnormalities | Other Comments |
| Angina | Usually | Restrosternal, radiating to arms, neck, back, or epigastrium | Squeezing, dull ache | Often with stress or exercise | 2–10 min up to 20–30 min | Occasionally dyspnea; dizziness and syncope rare | Often none. S4, occasionally | ECG often normal between attacks | Relieved by nitroglycerin |
| Acute myocardial Infarction | In some cases | Restrosternal, radiating to arms, neck, back, or epigastrium | Squeezing, dull ache, increase with time | No precipitating factor necessary | >30 min | Nausea and vomiting, diaphoresis, dyspnea | Heart failure, restlessness, shock; cardiac examination often normal | ECG may be diagnostic or normal | |








