Abstract
According to the United States Eye Injury Registry, eye injury is the leading cause of monocular blindness, and there are approximately 2.4 million eye injuries occurring annually in the US, resulting in 500,000 years of lost eyesight annually.1 These injuries occur more often in males (>70%), and 95% of occupational injuries occur in males.2,3 This chapter will describe the approach to the patient with eye trauma in the emergency department (ED), including how to perform a detailed history and physical examination related to eye injuries, as well as covering the traumatic presentations in Table 9.1.
Introduction and Epidemiology
According to the United States Eye Injury Registry, eye injury is the leading cause of monocular blindness, and there are approximately 2.4 million eye injuries occurring annually in the US, resulting in 500,000 years of lost eyesight annually.1 These injuries occur more often in males (>70%), and 95% of occupational injuries occur in males.2, 3 This chapter will describe the approach to the patient with eye trauma in the emergency department (ED), including how to perform a detailed history and physical examination related to eye injuries, as well as covering the traumatic presentations in Table 9.1.
Table 9.1 Eye trauma
| Vision-Threatening Conditions | Other Traumatic Eye Presentations |
|---|---|
|
|
There are multiple possible mechanisms for ocular trauma, outlined in Table 9.2.
Table 9.2 Mechanisms of ocular trauma
| Blunt | Penetrating | Other |
|---|---|---|
|
|
|
Approach to the Patient With Eye Trauma
Treat Life-Threatening Conditions First
Ocular trauma may be isolated or in combination with multisystem trauma. Given that there is a high association of ocular trauma with other facial trauma, the initial approach should focus on adequate airway management, if necessary, followed by respiratory and circulatory support. Once acute life threats are excluded, then history, examination, and intervention focus on the injured eye.
Involve the Ophthalmologist Early
It is important to involve the ophthalmologist early, as there is a higher chance for improved visual acuity with early involvement. In one study of serious injuries in 11,320 eyes, 27% of patients had initial visual acuity <20/200. However, with treatment, 61% of patients had improvements in their visual acuity.4 The authors noted specific positive and negative risk factors for improvement in visual acuity, detailed in Table 9.3.
Table 9.3 Factors associated with positive or negative visual acuity outcomes in traumatic eye injury
| Positive Risk Factors | Negative Risk Factors |
|---|---|
|
|
Focused History
The clinician should take a focused history, concentrating on the mechanism of injury to determine the likelihood of open vs. closed globe injuries. The timing of the injury should be elicited, as injuries that present early may have an improved chance of recovery and lower risk of infection or other complications compared to those that present later. Any associated symptoms should be noted, as they provide clues to the underlying injury. Diplopia, painful ocular motion, and facial numbness may indicate orbital wall fracture, while excessive tearing and photophobia may indicate traumatic iritis. Obtain any relevant information related to past ocular history, especially any previous surgical procedures, contact lens wear, and baseline visual status. For occupational injuries, document whether protective eyewear was being utilized at the time of injury – this may become an important medicolegal and/or worker’s compensation consideration. Finally, obtain relevant past medical history, active medications, allergies, and status of last tetanus immunization.
Immediately Identify Acute Visual Threats
In some cases, the history may lead the clinician to discover immediate threats to vision that require intervention prior to beginning a detailed examination of the eye. Examples include chemical injury requiring immediate irrigation, orbital compartment syndrome requiring lateral canthotomy/cantholysis, a protruding intraocular foreign body requiring stabilization and immediate referral without any further manipulation, and an open globe that may limit further aspects of the physical examination.
Examination of the Injured Eye
Visual Acuity
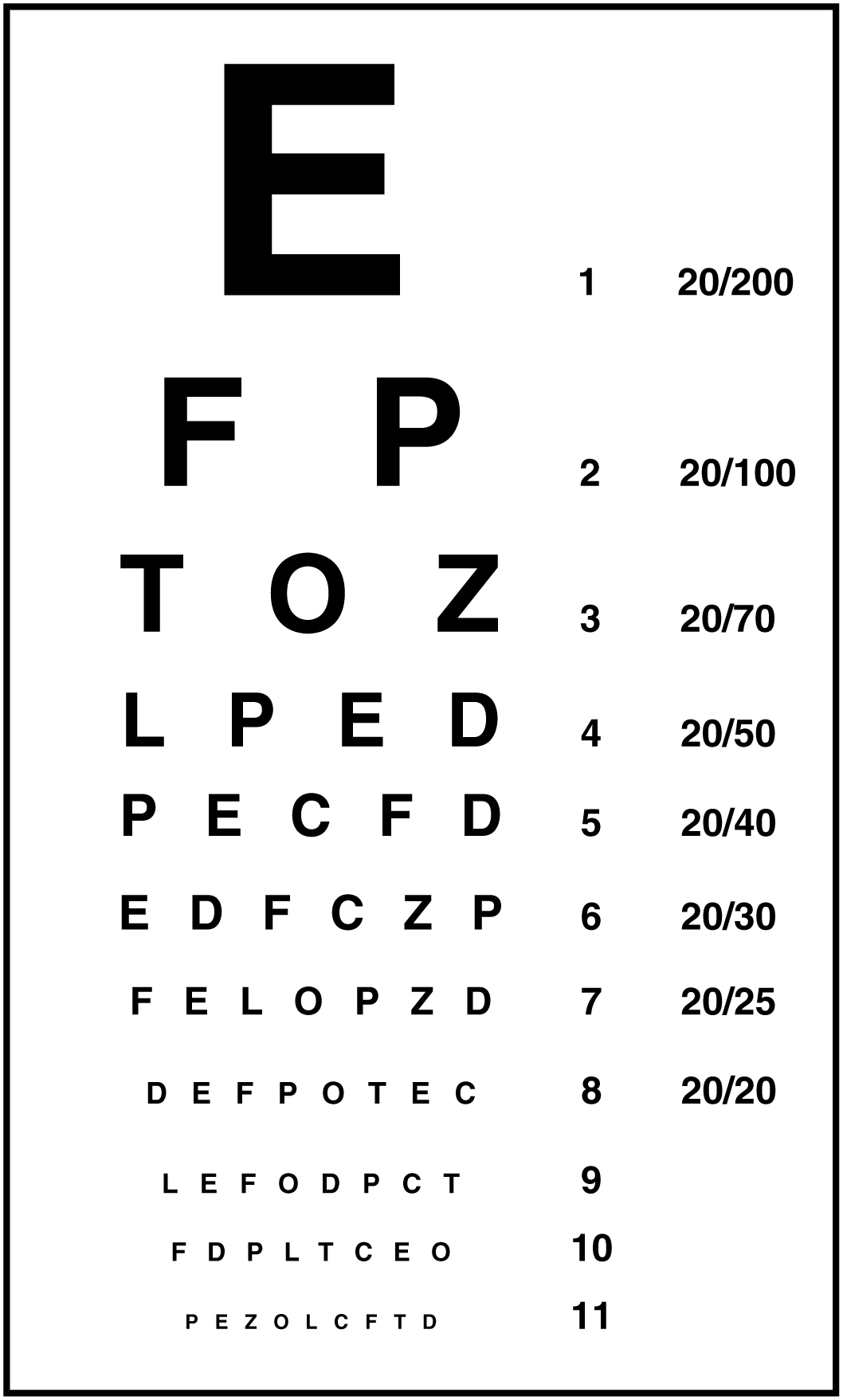
Visual acuity is often considered the primary “vital sign” of the eye. It should be performed on every ocular injury. Visual acuity is often obtained by use of a bedside “near card” or a Snellen Chart (Figure 9.1). Visual acuity should be tested with the patient’s corrective lenses in place, if possible. The clinician should test each eye individually. If the visual acuity is decreased to 20/40, worse than the patient’s baseline, or one line lower on the Snellen Chart compared to the patient’s baseline, then further evaluation and urgent Ophthalmology consultation are recommended.5

Figure 9.1 Snellen Chart as a visual acuity tool
Periocular Examination
It is critical to examine all structures surrounding the eye to identify any associated injuries that could lead to increased morbidity or dysfunction, such as orbital blowout fractures, nerve injuries, lacrimal system disruption, and many others. Evaluation should focus on the orbit, orbital rim, lids, lid function, and eyelid and periocular sensation.
Orbit and Orbital Rim
Palpate circumferentially around the orbit and along the orbital rim. Feel for step-off, crepitus, deformity, or elicitation of tenderness. Visually inspect for protrusion of any orbital fat through a wound, as this indicates damage to underlying levator muscle, orbital septum, or both.5
Lids and Lid Function
Visually inspect the superior and inferior lid and lid margin for any laceration, and give special attention to the area within 6–8 mm of the medial canthus – the expected location of the lacrimal canaliculi. In the case of suspected foreign body, the eyelid should be everted to examine the pretarsal sulcus of the upper lid, where foreign bodies tend to be retained. During evaluation of the lids, if the patient is unable to open the eyelids due to periorbital edema, then care should be taken to gently pull the lids apart or lift the upper lid and avoid exerting pressure on the globe. Additionally, evaluate whether the patient can effectively approximate the lids when closing them. Full-thickness eyelid lacerations are associated with ocular injury in two thirds of cases, and the clinician should have increased suspicion in those instances. The clinician can specifically evaluate for levator palpebrae transection by assessing for eyelid excursion. When the patient demonstrates upgaze, the upper lid will not elevate.5
Eyelid and Periocular Sensation
Evaluate sensation along the upper eyelid and forehead, as well as the lower eyelid and upper cheek. Any deficit in the superior aspect indicates a possible injury to the supraorbital nerve along the superior orbital rim. Any deficit in the inferior aspect indicates a possible injury to the infraorbital nerve, suggesting a possible inferior orbital wall fracture.
Ocular Examination
The ocular examination includes the pupils, extraocular motility, the anterior segment (conjunctiva, cornea, anterior chamber, iris, and lens), and the posterior segment (vitreous humor, retina, and optic nerve), as well as intraocular pressure measurement and fluorescein staining. Refer to Figure 9.2 for a review of relevant ocular anatomy.

Figure 9.2 Cross-sectional ocular anatomy
Pupils
Pupil examination is best conducted using a penlight to evaluate size, shape, and reactivity. The clinician should also evaluate for a relative afferent pupillary defect (rAPD). An rAPD is present when rapidly swinging the penlight to the affected eye causes the pupil to dilate, whereas shining the penlight into the unaffected eye will cause the pupil to constrict. This occurs due to either an optic nerve injury (e.g. traumatic optic neuropathy or avulsion), or possibly to a diffuse retinal injury such as a detachment. If a red reflex is symmetric, the rAPD is likely due to optic nerve injury. If a red reflex is asymmetric, the rAPD is likely due to posterior chamber pathology. A patient may have a pre-existing rAPD in cases of other severe ocular disease such as glaucoma or previous retinal detachment.
Extraocular Motility
The clinician should evaluate extraocular motion in the six cardinal directions of gaze, as well as symmetric gaze when looking straight ahead, up, and down. Figure 9.3 demonstrates the relevant movements with their associated ocular muscles. Asymmetries may be related to ocular muscle damage or entrapment, neuropathies, or retrobulbar hematoma.5

Figure 9.3 Six cardinal directions of gaze
Anterior Segment
While the slit lamp is the preferred method of evaluation of the anterior segment, it may not always be feasible. Significant associated trauma and patient condition may limit the evaluation of the anterior segment to that which can only be seen by penlight or Wood’s Lamp. Evaluation of the anterior segment should focus on the conjunctiva, cornea, anterior chamber, and iris.
Conjunctiva. The clinician should inspect the bulbar and the tarsal conjunctiva, evaluating for the presence or absence of subconjunctival hemorrhage, foreign bodies, chemosis, or laceration. Subconjunctival hemorrhage can be classified as flat or bullous, with the latter more suspicious for underlying scleral laceration. Foreign bodies are usually associated with tearing and photophobia. Chemosis appears as serous fluid within the substance of the conjunctiva. Conjunctival lacerations may also be associated with subconjunctival hemorrhages and chemosis and should raise suspicion for possible open globe or penetrating eye injury.
Cornea. The clinician should inspect the cornea for similar findings as the conjunctiva, including the presence of abrasions, foreign bodies, edema, and lacerations. Corneal abrasions are usually diagnosed through slit lamp examination but can be performed with fluorescein staining and Wood’s Lamp evaluation as an alternative.
Anterior chamber. The anterior chamber is best visualized with a slit lamp but can also be viewed with a penlight. The anterior chamber is the location of a hyphema, or a collection of red blood cells, in the setting of relevant trauma. A hyphema typically settles to the lower portion of the anterior chamber if the patient is upright for an extended period of time and can then be measured directly. With slit lamp, “cell and flare” may also be discovered, which suggests traumatic uveitis in the setting of trauma. Severe uveitis may result in hypopyon. The depth of the anterior chamber can be assessed by shining a penlight along the temporal portion of the chamber and visualizing the light shining across the flat iris in a normal anterior chamber, or only across a small portion of the temporal iris with a shadow across the nasal iris in a shallow anterior chamber. An asymmetric anterior chamber depth, when compared with the uninjured eye, can be a subtle sign of occult open globe injury.
Retina and Optic Nerve
The retina and optic nerve are best visualized through direct or panoramic ophthalmoscopy, but this can be technically difficult in the traumatized, undilated eye. In the absence of ophthalmoscopy, the red reflex can be used to grossly assess for retinal pathology. In the absence of a relative afferent pupillary defect, a uniform reflex that is symmetric between the two eyes can effectively exclude significant vitreous hemorrhage or large retinal detachments.5 Color vision testing with standard color plates is a sensitive indicator of optic nerve damage but is not typically performed in the ED. Red desaturation testing may also be helpful when traumatic optic neuropathy is suspected. Red desaturation is assessed by asking the patient to subjectively judge the relative intensity of a red colored object in one eye vs. the other.5,6
Intraocular Pressure Measurement
Prior to performing intraocular pressure (IOP) measurement, the clinician must exclude open globe injury, as placing pressure on the globe could further extrude intraocular contents. If open globe is ruled out, the clinician can measure IOP through applanation tonometry (i.e. TonoPen). Pressure should be obtained in both eyes for comparison. Normal IOP is between 10–21 mmHg. Increased IOP could be associated with orbital compartment syndrome, retrobulbar hematoma, hyphema, traumatic iritis, and with some chemical burns.
Fluorescein Staining
Fluorescein staining is performed in trauma to evaluate for corneal abrasions, lacerations, and Seidel sign. Fluorescein stain is placed through a drop or moistened strip on the conjunctiva and allowed to distribute across the surface of the eye through blinking. It is taken up by the basement membrane wherever an epithelial defect is present and illuminates under cobalt blue light. Seidel sign can be seen in penetrating trauma and is defined as a streaming of leaking aqueous humor through the fluorescein coating the ocular surface.5
Diagnostic Imaging
Computed tomography (CT) is the preferred imaging of choice in ocular trauma. It will effectively identify orbital wall trauma, soft tissue entrapment, fluid collection, and specific foreign bodies. Ultrasound can identify organic foreign bodies that may not appear on CT, but caution is recommended when utilizing ultrasound for intraocular assessment. Placing excessive pressure on the eye from the ultrasound probe may cause further extrusion of intraocular contents in an open globe injury. MRI is not the diagnostic imaging modality of choice in trauma due to the time to obtain the imaging, in addition to the contraindications in the presence of possible metallic foreign bodies. Refer to Table 9.4 for a summary of the imaging modalities with listed advantages and disadvantages.
Table 9.4 Advantages and disadvantages of ocular imaging modalities
| Computed Tomography | Ultrasound | Magnetic Resonance Imaging | |
|---|---|---|---|
| Advantages |
|
|
|
| Disadvantages |
|
|
|
Vision-Threatening Conditions
Ocular Chemical Burns
Ocular chemical burns are one of the few ocular traumas that require intervention prior to evaluation. Once an ocular chemical burn is identified, the area should immediately be flushed with 1–2 L of normal saline through manual application or a commercial irrigation system (i.e. Morgan Lenses) prior to evaluation. Irrigation should continue until the pH is neutral for at least 30 minutes after irrigation. Alkaline chemicals with pH >12 and acidic chemicals with pH <2 cause the most damage. However, alkaline chemicals cause more damage than acidic chemicals, due to the fact that alkaline chemicals cause liquefaction necrosis and deeper injury. In contrast, acidic chemicals cause coagulation necrosis, and the coagulum layer protects from further penetration. Table 9.5 lists some of the more common acids and bases implicated in ocular chemical burns.
Table 9.5 Common acids and alkalis that cause ocular chemical burns
| Acids (pH <7) | Alkalis (pH >7) |
|---|---|
|
|
Following irrigation, perform a detailed examination as described above, with particular attention to visual acuity, intraocular pressure, corneal scarring or clouding, anterior chamber “cell and flare,” and conjunctival injection and chemosis. Use of fluorescein staining can determine the presence of any epithelial defects (Figure 9.4).

Figure 9.4 Chemical injury to the eye. There is diffuse uptake of fluorescein dye, indicating a large corneal epithelial defect
Obtain ophthalmology consultation for all but minor burns. Any patient with corneal clouding or an epithelial defect after irrigation should receive prompt ophthalmology referral.7
Treatment of chemosis without corneal or anterior chamber findings is with erythromycin ointment four times daily and referral for ophthalmologic examination in 24 to 48 hours. Ensure that tetanus vaccination is updated, and provide adequate analgesics if epithelial defect is present.
Orbital Compartment Syndrome
Blunt ocular trauma can lead an orbital (intraconal or extraconal) hemorrhage, which may rapidly elevate orbital pressure, transmitting pressure to the globe and optic nerve, and leading to ischemia and eventual blindness if not corrected in a timely fashion. It is important to distinguish preseptal from postseptal hemorrhage, given the clinical significance of the latter. Key history and physical exam findings are outlined in Box 9.1.
Box 9.1 Key History and Physical Exam Findings of Orbital Compartment Syndrome
Acute onset decreased vision
Diplopia
Eye pain
Periorbital swelling
Afferent pupillary defect
Intraocular pressure >40 mmHg
Restricted ocular motility
Proptosis
Diffuse subconjunctival hemorrhage
The most important tool for the emergency physician is high index of suspicion and a low threshold to take action and enlist help of an ophthalmologist. The diagnosis is made through use of tonometry, measuring intraocular pressures greater than 40 mmHg. Additionally, CT of the orbit can reveal retrobulbar or intraorbital hemorrhage as the source of the elevated pressures (Figure 9.5).

Figure 9.5 CT scan showing right retrobulbar hemorrhage in the intraconal space, causing right proptosis and a visible “tenting” of the globe where the optic nerve is connected
If orbital compartment syndrome is suspected, emergency ophthalmology consult should be requested. Management of orbital compartment syndrome is through emergent lateral canthotomy and inferior cantholysis, which reduce globe and intraocular pressure and reestablish retinal artery blood flow.7 Outside of delay for ABC’s of trauma resuscitation, there should be no other delays, including for imaging. The steps for lateral cantholysis are presented in Box 9.2.
Box 9.2 Steps For Lateral Canthotomy and Inferior Cantholysis8
1. Cleanse the area with povidone-iodine solution, hibiclense, or alcohol.
2. Using a 25 g needle, perform field block with infiltration of 1% or 2% lidocaine with epinephrine above and below the lateral canthus 1–2 cm.
3. Clamp a straight hemostat horizontally at the lateral canthal crus (between the upper and lower eyelid) for approximately 1 minute. This helps with hemostasis.
4. Remove the clamp, and with blunt-tipped scissors, cut between the upper and lower eyelid at the lateral canthus approximately 1 cm (called a lateral canthotomy).
5. Grasp the lower lid at the lid margin with forceps (i.e. Adsons) and provide upward traction toward the ceiling.
6. Identify the lateral canthal tendon with a strumming motion using closed scissors.
7. Once identified, cut the tendon until the eyelid is fully mobile (called an inferior cantholysis). The procedure is successful if the lateral lower eyelid can be mobilized to the superolateral orbital rim and to the temporal limbus.
8. Reassess visual acuity and intraocular pressure immediately after the procedure.
9. If intraocular pressure remains elevated, a superior cantholysis is needed. Identify and cut the superior crus of the canthal tendon.
10. Continue to provide hemostasis through direct compression of the wound at the orbital rim without further compression of the globe itself. Bipolar cautery may need to be used if bleeding at the canthotomy incision cannot be controlled.
After lateral canthotomy and inferior cantholysis, further management of orbital compartment syndrome includes elevation of the head of bed to 45°, pain control, correction of coagulopathy, management of elevated blood pressure after analgesia, prevention of sudden increases in intraocular pressure through use of antiemetics and cough suppression, and hospitalization for definitive management.
Carotid-Cavernous Fistula
An additional vision-threatening diagnosis as a result of blunt trauma is a carotid cavernous fistula (CCF). Seen in up to 4% of basilar skull fractures and other blunt facial trauma, a direct, high-flow CCF results from a direct connection between the carotid artery and the surrounding cavernous sinus.9,10 Symptoms may manifest immediately or be delayed by days to weeks.9 Symptoms are usually sudden in onset when they do occur and are the result of arterialization of orbital and ocular venous systems. Signs and symptoms are included in Box 9.3.9, 11–13
Box 9.3 Signs and Symptoms of Carotid-Cavernous Fistula With Associated Percent of Patients With Findings
Subjective bruit (80%), bruits may also be auscultated over the globe
Blurred vision (25–29%)
Headache (53–75%)
Diplopia (50–85%)
Ocular and/or orbital pain (35%)
Proptosis (72–87%)
Chemosis and conjunctival injection (55–89%)
Cranial nerve VI palsy (50–85%)
Cranial nerve III palsy (67%)
Cranial nerve IV palsy (49%)
Fundoscopic exam findings including dilated retinal veins and intraretinal hemorrhages
The arterialization of conjunctival and episcleral vessels results from blood forced into the venous drainage of the orbit, leading to elevated episcleral venous pressure (Figures 9.6a and 9.6b), secondary glaucoma, and, rarely, catastrophic central retinal artery occlusion.9, 14










{kind=link}
