John J. Graykoski A stroke is an interruption of blood circulation to the brain causing a neurologic deficit that reflects the area of the brain affected. A stroke can be ischemic or hemorrhagic.1 Ischemic stroke is most prevalent. It is occlusive in nature. Lacunar strokes are seen more in older adults and diabetic patients. They affect smaller areas of the brain by closing off arterioles. Hemorrhagic stroke has a lower incidence than ischemic stroke but is more deadly. Transient ischemic attacks (TIAs) are neurologic deficits that resolve completely within a few hours but no more than 24 hours. A TIA is part of a spectrum ending in acute ischemic stroke, referred to collectively as an acute cerebrovascular syndrome (ACVS) which reflects the growing awareness that stroke can be the end result of TIA. More aggressive management of TIA, including neurologic consultation and hospitalization, can reduce the risk of more devastating stroke.1 Ischemic strokes tend to occur in older patients with other disease processes, whereas hemorrhagic strokes typically occur in healthy individuals between the ages of 40 and 60 years. Risk factors for ischemic stroke include hypertension, older age, cigarette smoking, male gender, family history, race, previous stroke or TIA, carotid stenosis of more than 80%, atrial fibrillation, and drug abuse. Other factors that may contribute are diabetes, obesity, sedentary lifestyle, and elevated serum cholesterol. Stroke is now the fifth most common cause of death in the United States. This is an improvement from being the third most common cause only a few years ago. The decrease is in large part a result of how stroke is managed (see the Management section). Every year, 795,000 people in the United States have a stroke; stroke kills 130,000 per year.2,3,4 There are racial disparities in stroke occurrence; both black men and black women are twice as likely as other races to have a first stroke, and more likely to die.3 Stroke remains a leading cause of disability in the United States, with significant social and financial implications for families and society. The cost of stroke care is estimated to be $36.5 billion dollars annually. Stroke also represents a significant burden for long-term care. Fifty percent to 70% of stroke survivors regain functional independence, but 15% to 30% are permanently disabled. Institutional care is required by 20% at 3 months after onset. Ischemic stroke is the most common type of stroke. In a thrombotic event, a critical degree of atherosclerosis causes complete or relatively complete blockage of blood flow through a local area. In an embolic event, a clot forms elsewhere (e.g., a fibrillating atrium), breaks off, and travels through the arterial circulation until it lodges in a vessel and blocks the flow of blood distally. The effects of arterial occlusion on brain tissue vary, depending on the location of the occlusion in relation to available collateral and anastomotic channels and the degree and duration of the ischemia. The specific neurologic deficit relates to the location and size of the infarction or focus of ischemia. At the time of arterial occlusion, the viscosity of the blood and resistance to flow both increase, and there is sludging within the vessels. The tissue becomes pale. If the ischemia is prolonged, sludging and endothelial damage prevent normal reflow. Cellular breakdown and swelling occur.5 Thirteen percent of all strokes are the results of brain bleeds.5 There are two types of hemorrhagic stroke: subarachnoid and intracerebral. A subarachnoid bleed occurs in the subarachnoid space, the area between the tissue that covers the brain and the brain. These are usually caused by an aneurysm, arteriovenous malformation, or an inherited bleeding disorder. Risk factors include smoking, hypertension, connective tissue disorders, other known aneurysms, and polycystic kidney disease. Family history may play a role.5 Anticoagulation with warfarin and antiplatelet therapy increase the risk of brain bleed in individuals taking those medications, especially with head injury. Intracerebral hemorrhage is caused by a weakened artery in the brain. Uncontrolled hypertension is the most common cause of the vessel weakening. Other contributing risks include smoking, obesity, high-fat diet, and drugs, including cocaine.6 In either embolic or hemorrhagic stroke, an area immediately surrounding the injury dies within a few minutes from lack of oxygen and the failure of the oxygen-dependent adenosine triphosphate (ATP) metabolic pathway. In a broader area of injury, referred to as the penumbra, the damage is more dynamic, extending for 12 to 24 hours. It is believed the release of intracellular calcium initiates the sequence of programmed cell death, or apoptosis.6 Patients with ACVS (TIA and strokes) have a similar presentation, although time is a major differentiating factor. The symptoms of cerebral ischemia are widely variable and depend on the vascular territory involved. When the carotid artery circulation is involved, the symptoms reflect ischemia to the ipsilateral eye or brain. The classic visual disturbance (amaurosis fugax) is a transient, painless loss of vision, often described as a shade descending over the visual field. Hemispheric brain ischemia usually causes weakness or numbness of the contralateral face or limbs. Language difficulties and cognitive and behavioral changes may also occur. Vertebrobasilar ACVS (TIA) and strokes may manifest with vertigo, nystagmus, diplopia, dysconjugate gaze, or deficits of cranial nerves III to XII. Many signs and symptoms are common to strokes affecting both anterior (carotid) and posterior (vertebrobasilar) circulation. These include hemiparesis, hemisensory loss, visual field defects, ataxia (difficulty with balance and coordination), dysarthria (difficulty speaking), reflex asymmetry, and Babinski sign. Headache does not usually occur in ischemic stroke but is common in hemorrhagic stroke. When it is present, headache is not nearly as severe as in intracerebral or subarachnoid hemorrhage, and the neck is not stiff. ACVS (TIA) more commonly precedes ischemic stroke than hemorrhagic stroke. In ischemic stroke, the patient usually has a single attack, and the entire illness evolves within a few hours. However, the stroke may occur in a “stuttering” fashion, with intermittent progression of neurologic deficits that extends for several hours, a day, or longer. A partial stroke may occur and even recede temporarily for several hours, after which there may be rapid progression to the full-blown stroke. The stroke may involve several parts of the body at once or only one part (e.g., a limb or one side of the face), with the other parts becoming involved in a stepwise fashion until the stroke is fully developed. The stroke may occur during sleep, with the patient remaining unaware until he or she tries to get up and discovers the paralysis. In subarachnoid hemorrhage, the clinical presentation is usually heralded by the abrupt onset of a severe headache (“the worst headache of my life”), nausea and vomiting, signs of meningeal irritation, and varying degrees of neurologic dysfunction. Loss of consciousness at the time of the initial event is common but is usually short-lived. Nearly 50% of patients with aneurysmal subarachnoid hemorrhage give a history of atypical headaches occurring days to weeks before the definitive event. These sentinel headaches are characteristically sudden in onset and are often associated with nausea, vomiting, and dizziness, with or without neurologic dysfunction. Some hemorrhagic events may manifest with seizures. Patients with hypertensive intracerebral hemorrhage may have no consistent warning or prodromal symptoms. In the majority of cases, the hemorrhage has its onset while the patient is up and active; onset during sleep is rare. The blood pressure is elevated in almost all cases. The neurologic signs and symptoms vary with the site and size of the extravasation of blood. The patient may lapse almost immediately into stupor and coma, with hemiplegia and steady deterioration to death during the next several hours. More often, the patient complains of a headache, followed within a few minutes by unilateral facial sag, slurred speech, weakness in an arm and leg, and eye deviation away from the paretic limbs. These events, occurring during a period of 5 to 30 minutes, strongly suggest intracerebral bleeding. More advanced cases are characterized by paralysis, aphasia, stupor, coma, deep and irregular respiration, dilated and fixed pupils, and, occasionally, decerebrate rigidity. Findings on physical examination correspond to the location of the vascular event and associated neurologic deficit. Initial attention should always focus on a patent and protected airway, a good respiratory effort, and a competent heart rate with good peripheral circulation (ABCs of advanced clinical life support). A complete neurologic examination to assess areas of deficit should quickly follow. Because ACVS (TIA) precedes 7.1% of all strokes,7 a risk stratification tool should be used to guide treatment for ACVS (TIA). The ABCD2 score (Table 191-1) is valuable for this purpose.8 TABLE 191-1 ABCD2 Score for Acute Cerebral Vascular Syndrome (Transient Ischemic Attack) Diagnostic studies are necessary to determine the type of stroke and the probable cause as well as to detect complications. Because management is vastly different, it is important to be able to quickly differentiate ischemic stroke from hemorrhagic stroke and to exclude disorders that may occasionally resemble stroke. A head computed tomography (CT) scan is the most common initial imaging procedure. A noncontrast CT scan is better than magnetic resonance imaging (MRI) in discriminating between hemorrhagic and ischemic stroke. Patients who have atypical presentations or who have unusual findings on noncontrast CT scans ought to have a CT scan with contrast enhancement or MRI to exclude tumor. CT can miss small subcortical or cortical infarctions or lesions in the posterior fossa. Among patients with ischemic stroke, the CT scan may be normal in the first few hours but will usually show abnormalities after 12 hours or more. In hemorrhagic stroke, the head CT scan will usually be abnormal at presentation to the emergency department. If the initial CT scan shows hemorrhage, other studies (e.g., arteriography) may be necessary to determine whether an underlying vascular malformation is present. In certified stroke centers, the time from presentation in the emergency department to CT is a measured statistic, with the goal of making a determination on the use of thrombolytics within the 3- to 4.5-hour window when most eligible candidates could benefit. Other diagnostic studies include an electrocardiogram (ECG), chest radiography, pulse oximetry or arterial blood gas (ABG) assessment, complete blood count (CBC) with platelets, prothrombin time (PT), partial thromboplastin time (PTT), serum glucose concentration, creatinine level, blood urea nitrogen (BUN) level, and electrolyte values. Doing these tests should not delay the CT scan; time is of the essence, and in specialty stroke centers the clock is literally ticking. Depending on the clinical presentation, other tests may be necessary, including examination of the cerebrospinal fluid if central nervous system infection is suspected or when the clinical picture suggests subarachnoid hemorrhage but the head CT scan is normal. Electroencephalography (EEG) is indicated when the clinical picture suggests seizure. Carotid ultrasonography will assess patency of the carotid arteries. Carotid arteriography or magnetic resonance angiography should be done in patients with severe carotid stenosis on ultrasound evaluation who are considered candidates for endarterectomy. Transesophageal echocardiography and Holter monitoring may be performed if the presentation is suggestive of an embolic event originating from the heart. Other laboratory tests that may be indicated include serum cholesterol level, toxicology screening, erythrocyte sedimentation rate (ESR), hemoglobin electrophoresis, fibrinogen level, serum protein electrophoresis, antiphospholipid antibody level, serologic test for syphilis, protein C level, protein S level, antithrombin III level, lupus anticoagulant, anticardiolipin antibody level, and connective tissue disease screen. Diagnostics Cerebrovascular Events Other Diagnostics The following are tests to consider after emergency care, stabilization, and treatments.
Cerebrovascular Events
Definition and Epidemiology
Pathophysiology
Ischemic Stroke
Hemorrhagic Stroke
Clinical Presentation
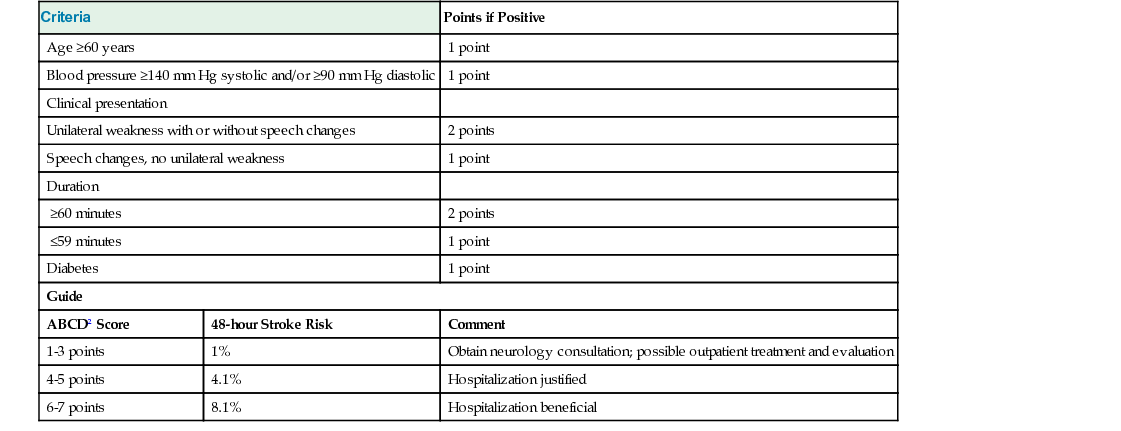
Physical Examination
Criteria
Points if Positive
Age ≥60 years
1 point
Blood pressure ≥140 mm Hg systolic and/or ≥90 mm Hg diastolic
1 point
Clinical presentation
Unilateral weakness with or without speech changes
2 points
Speech changes, no unilateral weakness
1 point
Duration
≥60 minutes
2 points
≤59 minutes
1 point
Diabetes
1 point
Guide
ABCD2 Score
48-hour Stroke Risk
Comment
1-3 points
1%
Obtain neurology consultation; possible outpatient treatment and evaluation
4-5 points
4.1%
Hospitalization justified
6-7 points
8.1%
Hospitalization beneficial
Diagnostics







