1 Cardiovascular system
Anaesthesia and cardiac disease
Previous ischaemia
Important risk studies
Investigations
ECHO. Ejection fraction, wall motion and valve abnormalities.
Technetium-99m scan. Similar to thallium scan but underperfused areas show as hot spots.
General anaesthesia for non-cardiac surgery
Choice of anaesthetic technique or volatile agent has no proven effect on cardiac outcome. Aim to optimize myocardial oxygen balance (Table 1.1).
Table 1.1 Factors affecting oxygen supply and demand
| Supply | Demand |
|---|---|
| Coronary perfusion | Preload (LVEDP) |
| O2 content | Afterload (SVR) |
| Heart rate | Heart rate |
| Contractility |

Premedication
Aspirin. Although aspirin increases the risk of bleeding complications, it does not increase the severity level of the bleeding complication. A meta-analysis has shown that aspirin withdrawal was associated with a three-fold higher risk of major cardiac events (Biondi-Zoccai et al 2006).
Anaesthetic
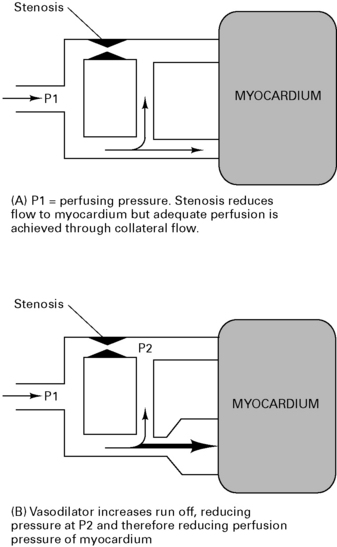
Volatiles. Enflurane and halothane both decrease coronary blood flow, but isoflurane, sevoflurane and desflurane increase coronary blood flow and maintain LV function in normotensive patients. Tachycardia with isoflurane increases myocardial work, but this is minimal with balanced anaesthesia. There is some concern that isoflurane may cause coronary steal (Fig 1.1) but it is thought not to do so as long as coronary perfusion pressure is maintained. There is growing evidence that isoflurane has myocardial protective properties, limiting infarct size and improving functional recovery. This mechanism mimics ischaemic pre-conditioning and involves the opening of ATP-dependent K+ channels causing vasodilation and preservation of cellular ATP supplies. Desflurane and sevoflurane probably have similar but less marked cardioprotective effects.
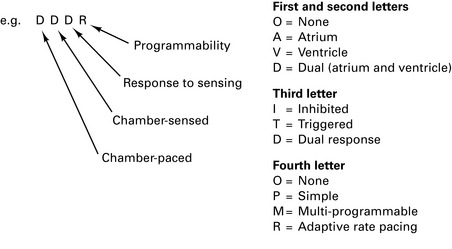
Pacemakers
There are 200 000 patients with implanted pacemakers in the UK.
Automatic implantable cardioverter defibrillators (AICDs)
Atrial Fibrillation: the Management of Atrial Fibrillation
National Institute for Health and Clinical Excellence, June 2006
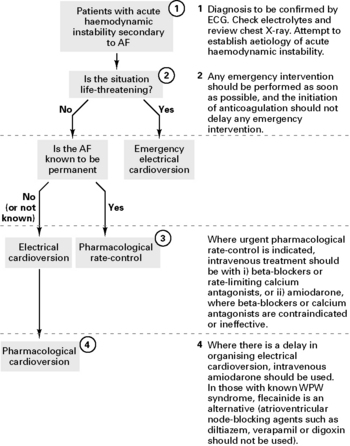
Antithrombotic therapy for acute-onset atrial fibrillation (AF)
For patients with acute AF who are receiving no, or only sub-therapeutic anticoagulation therapy:
Anaesthetic considerations for heart surgery
Ischaemic heart disease
Rate pressure product (RPP) = heart rate × systolic pressure. Aim to maintain value at below 12 000.
Endocarditis prophylaxis
National Institute for Health and Clinical Excellence, March 2008 (http://www.nice.org.uk/nicemedia/pdf/CG64PIEQRG.pdf)
Summary
Risk factors for the development of infective endocarditis
Related posts:






Full access? Get Clinical Tree


